J. Lacy Kamm
Sesamoid Fracture
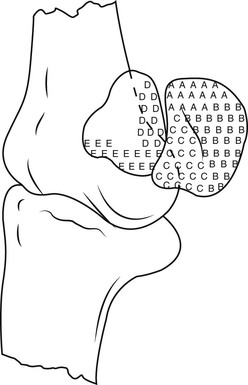
The proximal sesamoid bones (PSBs) are paired small pyramid-shaped bones on the palmar and plantar surface of the metacarpophalangeal and metatarsophalangeal joints, respectively. The most proximal portion of the bone is called the apex, the midportion is called the body, and the most distal portion is called the base. Surfaces of the proximal sesamoid bones include the articular surface, the abaxial surface, the axial surface, and the basilar surface (Figure 195-1). The bones contain cortical and cancellous bone, with the densest portion of trabecular bone arising at about one third the distance from the apex to the base.
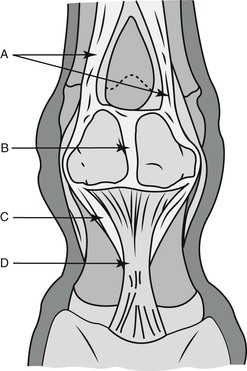
The proximal sesamoid bones are a component of the suspensory apparatus (Figure 195-2). The suspensory apparatus serves two main purposes: it prevents hyperextension of the metacarpophalangeal and metatarsophalangeal joints and converts energy from impact into energy for push-off, functioning like a trampoline. This conversion of energy is facilitated by the elasticity of the suspensory ligament. The suspensory apparatus includes the suspensory ligament, proximal sesamoid bones, and distal sesamoidean ligaments. The suspensory ligament originates at the proximal aspect of the third metacarpal and metatarsal bones and inserts on the apical and abaxial component of the PSBs. The distal sesamoidean ligaments include the short, cruciate, oblique, and straight sesamoidean ligaments. These originate at the basal surface of the PSBs and insert on the proximal and middle phalanges. An intersesamoidean ligament runs between the axial surfaces of the sesamoid bones and, along with the joint capsule and the tendon sheath, divides the metacarpophalangeal and metatarsophalangeal joints from the digital flexor tendon sheath. Collateral sesamoidean ligaments, along with the proximal annular ligament, provide stability to the joint by attaching the sesamoids to the medial and lateral aspects of the third metacarpal and metatarsal bones.
Diseases of the PSBs occur primarily in racehorses, most often in young racehorses in the early period of training. This is because of the slow maturation of the proximal sesamoid bones, compared with the suspensory ligament. With exercise, the suspensory ligament quickly strengthens. In one cadaver study in which the suspensory apparatus was tested by exerting force until the point of failure in exercised or pastured horses, the force needed to achieve failure was significantly greater in the exercised group, compared with the pastured group. Additionally, failure occurred at the level of the proximal sesamoid bone more commonly in the exercised group than in the pastured group. These findings support the thought that the suspensory ligament strengthens more than the proximal sesamoid bones in response to exercise.
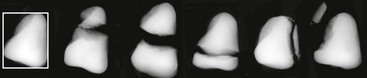
Diseases of the proximal sesamoid bones include fracture, sesamoiditis, enthesiophytes, and osteophytes. Septic osteitis can develop and does so most commonly in conjunction with a septic metacarpophalangeal or metatarsophalangeal joint. Fracture types include apical, abaxial, axial, midbody, and basilar (Figure 195-3). These diseases are described in detail in the following sections.
Diagnosis
Diagnosis of PSB lesions may begin with perineural anesthesia. A basisesamoid or abaxial block may partially anesthetize the sesamoids by proximal diffusion of the anesthetic, although the lameness is usually only mildly improved. A low four-point block will more completely remove pain originating in the sesamoids. Imaging of the sesamoids can be obtained with metacarpophalangeal or metatarsophalangeal joint radiographs and with ultrasound of the suspensory branches and the distal sesamoidean ligaments. Horses often have some degree of metacarpophalangeal or metatarsophalangeal joint effusion and lameness ranging from mild to severe.



