Melissa Sinclair
Sedation and Anesthetic Management of Foals
Sedation and anesthesia of foals is necessary for a variety of reasons, ranging from the need to obtain radiographs or undertake other minor elective procedures to emergency exploratory laparotomy for colic or uroabdomen. In either type of situation, preexisting conditions such as pneumonia, hypoxemia, and dehydration can further complicate the anesthetic management. Foal anesthesia can be challenging, and the overall relative risk is associated with foal age and the procedure. Foals pose a unique challenge because they are physiologically different from other neonatal animals and also from the mature horse. Safe sedation and anesthesia of foals requires that practitioners consider the challenges posed by some of the unique physiologic features of the equine neonate.
Specific Neonatal Considerations
Risk for Anesthesia in Neonatal and Juvenile Foals
Foals are grouped as neonates from birth until 1 month of age and as juveniles from 1 to 3 months. Special considerations for sedation and anesthesia are given to the very young neonatal foal (<7 to 10 days), especially if signs of prematurity are evident. Foals older than 3 months of age are generally treated as young adult horses in terms of drug, equipment, and recovery requirements.
A two-part study (the Confidential Enquiry Into Equine Perioperative Fatalities [CEPEF] study) revealed that foals younger than 1 week of age, anesthetized for procedures other than colic, were 7.3 times as likely to die as horses 4 to 8 years of age that underwent elective procedures. By 1 to 4 weeks of age, this risk was 2.02 times as likely, and by 1 to 3 months was similar (0.9 times as likely) to that in the general equine population. These increased risks are likely related to the physiology of the neonate, the effect of neonatal physiology on drug pharmacokinetics, and the anesthetic regimens used in foals. Despite the impact of age on the morbidity and mortality rates, few studies have compared the effects of anesthetic regimens in foals younger than 1 week of age.
Physiology of the Foal
Respiratory System
At birth, foals have a low Pao2 (about 56 mm Hg), which gradually increases to 85 to 90 mm Hg by 1 week and then to the normal range of 95 to 100 mm Hg after 1 week. In the first hour of life, foals have a high tissue oxygen demand (7 to 10 mL/kg/minute), which decreases to 5 mL/kg/minute by 12 hours. Their respiratory rate of approximately 70 breaths/minute at birth slows to 40 to 50 breaths/minute by 1 week. Because of the overall poor tone of foals’ respiratory muscles, compliant chest, and low lung volume at the end of expiration, foals are prone to hypoventilation and hypoxemia, which is further exacerbated by sedation and general anesthesia. For this reason, oxygen administration during sedation and recumbency is warranted in the neonatal foal.
Cardiovascular System
The cardiovascular system of the foal differs from that of the adult horse but does not fit all generalizations from other neonatal animals. The mean heart rate of foals decreases from 100 beats/minute at birth to 70 beats/minute by 2 months, and to 50 beats/minute at 3 months of age. Systolic heart murmurs (less than grade 2 on a scale of 1 to 5) restricted to the left heart base may be normal in foals until 3 months of age and are usually related to blood flow through a still-patent ductus arteriosus. Vagal influences predominate in control of the neonatal myocardium; sympathetic innervation is sparse, and the heart’s response to adrenergic drugs is diminished, so larger doses of the latter may be indicated. The ventricle has fewer contractile elements and more connective tissue, resulting in lower compliance and overall strength of contraction. The low compliance limits the potential to increase stroke volume, which has two important consequences: cardiac output is strongly influenced by heart rate, and increases or decreases in preload and afterload are poorly tolerated so that even small volumes of blood loss (e.g., 5 mL/kg) are clinically significant.
Between birth and 2 weeks of age, cardiac output increases and systemic vascular resistance decreases in foals. Two hours after birth, systemic vascular resistance (dynes · sec · cm−5) is 1027, but by 12 days it decreases to 520, a value that is higher than that of adult horses (230 to 250). Despite the high resistance, arterial blood pressure (96 to 100 mm Hg) is consistently lower in foals than in adults (120 mm Hg). Foal blood pressure can vary slightly depending on foal position, on whether the measurement is taken by direct or indirect means (Doppler versus oscillometric), or on the basis of breed (ponies’ pressures are lower than those in Thoroughbreds). To summarize cardiovascular findings in foals, arterial blood pressure is lower in foals than in adult horses, but not excessively. Cardiac output is higher because of a higher heart rate, but systemic vascular resistance is not lower than in the adult horse.
Drug Dosage and Metabolism
Foals younger than 7 days of age can be more sensitive to the effects of anesthetic drugs than older animals because of increased transfer of drug across the blood-brain barrier (BBB) and altered rates of drug disposition, metabolism, and excretion. The immature BBB of young foals can result in a more rapid and profound response to sedative agents, such as benzodiazepines, α2-receptor agonists, and opioids. The hypoalbuminemia characteristic of foals younger than 8 weeks results in less protein binding of anesthetic agents and increased quantities of active unbound anesthetic, which can cross the BBB to cause an overall greater effect despite accurate dose calculations. This effect is most obvious with highly protein-bound agents such as diazepam, which is 98% protein bound.
At birth, foals have a high body water content, compared with adult horses. The higher body water content of neonatal foals increases the volume of distribution of injectable anesthetic drugs so that neonates require a greater dose of drug to achieve a given response during induction. However, because of the higher permeability of the BBB and reduction in drug binding by albumin, this higher dose can result in a more profound drug effect.
By 3 to 4 weeks of age, the foal’s hepatic metabolic pathways are well developed. However, in foals younger than 7 to 10 days of age, anesthetic drugs relying on the liver for metabolism (e.g., thiobarbiturates, ketamine, and acepromazine) should be used cautiously unless they are reversible (opioids, benzodiazepines). In these young foals, the hepatic enzyme systems function at a lower capacity, resulting in prolonged sedation or anesthesia and recovery, an effect that may warrant reversal when possible. In the author’s experience, this is most common with benzodiazepines, especially in premature foals. From the viewpoint of drug elimination, foal kidneys are mature at 4 days of life.
Laboratory Values
Hemoglobin concentration and packed cell volume (PCV) decrease from values in the range of 15.4 g/dL and 43%, respectively, at birth to 12.6 g/dL and 34% at 2 weeks of age. Hemoglobin concentrations decrease because of a low rate of erythrocyte production, shorter erythrocyte life span, and hemodilution by an expanding plasma volume. Hematopoiesis begins at 6 to 12 weeks, making foals 2 to 8 weeks of age susceptible to anemia.
Total protein values are in the range of 48.3 ± 2.3 g/L (4.8 ± 0.23 mg/dL) at birth, increase to reference range (60 to 65 g/L [6 to 6.5 mg/dL]) by 1 to 4 weeks of age, and remain stable thereafter. Earlier reports in foals sampled at birth noted a lower mean blood urea nitrogen of less than 5.7 mg/dL (2 mmol/L) up to 3 months of age, which increased to normal mean adult values (10 mg/dL [3.5 mmol/L]) thereafter. Compared with other species, foals excrete dilute urine. Low blood urea nitrogen concentrations are normal in foals until 3 months of age because of rapid incorporation of amino acids into proteins.
Anesthetic Preparation and Techniques
Fasting
Because newborn foals have low liver glycogen stores, prolonged withholding of nursing is not recommended. Preventing nursing for 15 to 30 minutes before anesthesia is acceptable for foals younger than 1 month of age because, in the absence of gastrointestinal obstruction, regurgitation and development of intestinal tympany are not common. For foals 1 to 3 months of age, fasting for 2 to 6 hours is generally recommended.
Sedation
Sedatives alone may be used for diagnostic or minor procedures or before induction of general anesthesia (Table 182-1). The disease and condition of the foal, along with its age and temperament, dictate drug selection and dose. Despite the ability of several classes of drugs to provide good levels of sedation and restraint in foals, attention should be paid to which agents are also analgesics. Analgesic agents and local anesthetic techniques should always be used in foal sedative and general anesthetic protocols. Oxygen supplementation should be available during profound or prolonged sedation alone in foals.
TABLE 182-1
Sedative Agents Used in Foals
| Drug | Neonatal Foal <10 days of age | Juvenile Foal 10 days-1 mo of age | Juvenile Foal 1-3 mo of age |
| Benzodiazepines | |||
| Diazepam, IV Midazolam, IV or IM | 0.02-0.1 mg/kg 0.02-0.1 mg/kg | 0.02-0.1 mg/kg 0.02-0.2 mg/kg | 0.02-0.04 mg/kg 0.02-0.04 mg/kg |
| Opioids | |||
| Butorphanol, IV or IM | 0.02-0.1 mg/kg | 0.02-0.1 mg/kg | 0.02-0.04 mg/kg |
| α2 Agonists | |||
| Xylazine, IV or IM Romifidine, IV or IM Detomidine, IV or IM | 0.1-0.2 mg/kg† 0.02-0.03 mg/kg† 0.002-0.003 mg/kg† | 0.1-0.5 mg/kg* 0.02-0.05 mg/kg* 0.003-0.08 mg/kg* | 0.02-0.8 mg/kg* 0.02-0.1 mg/kg* 0.005-0.1 mg/kg* |
| Phenothiazines | |||
| Acepromazine, IV or IM | Not recommended | 0.01-0.02 mg/kg | 0.02-0.04 mg/kg* |
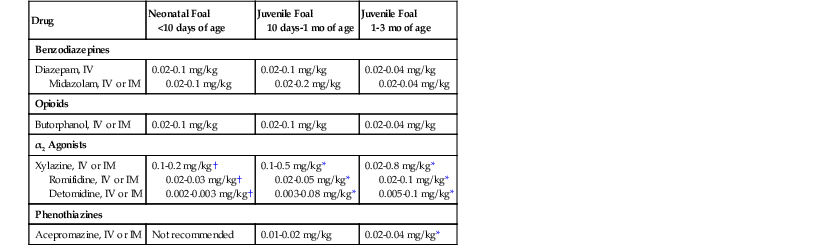
* Higher doses are typically given by the IM route.
† Low dose only if other sedatives do not work. Not recommended in sick foals.
Foals Younger Than 10 Days
The most common sedative agents used in foals younger than 10 days are benzodiazepines and the agonist-antagonist opioid butorphanol (µ-receptor antagonist and κ-receptor agonist). Both provide good sedation, are reversible if excessive sedation or hypoventilation occurs, and have minimal cardiovascular effects. The negative cardiovascular effects associated with α2-agonists or acepromazine make both a poor choice in this age group. α2-Agonists also increase pulmonary vascular resistance, which could potentially reopen the fetal circulation, leading to a right-to-left cardiac shunt and hypoxemia in the newborn foal, although this has not been documented in the literature.
For minor procedures such as the taking of radiographs, benzodiazepines (diazepam, 0.01 to 0.1 mg/kg, IV, or midazolam, 0.01 to 0.1 mg/kg, IV or IM) provide good sedation, but they do not provide analgesia. Because both these drugs cause muscle relaxation and recumbency at higher doses, foals should be supported while being sedated and should be assisted into recumbency. Both benzodiazepines can be reversed with flumazenil (0.01 to 0.025 mg/kg, IV to effect, or IM). In general, 1 mg of flumazenil can reverse 10 mg of diazepam or midazolam. The flumazenil is diluted in saline and given slowly intravenously to reach the desired endpoint and minimize the chance of excitement. In the absence of venous access, IM doses can be administered.
If additional sedation or analgesia is necessary, butorphanol (0.05 to 0.2 mg/kg, IV or IM) can be combined with the benzodiazepine, or it may be used on its own. Doses of 0.05 mg/kg IV or IM induce sedation, decrease respiratory rate, decrease borborygmus, and increase suckling behavior, but have no major adverse effects. However, at least 0.1 mg/kg is required to produce analgesia in recent studies. Overall, butorphanol at these doses can be used safely in foals and has minor cardiorespiratory effects. Butorphanol can be antagonized with naloxone (0.01 to 0.04 mg/kg, IV or IM) if excessive sedation persists. Titration of naloxone IV to effect is preferred to maintain a level of opioid analgesia. This is done by adding 1 mL (0.4 mg) of naloxone to 10 mL saline and titrating administration at 0.5 to 1 mL every 2 to 3 minutes intravenously until the appropriate level of arousal is achieved.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


