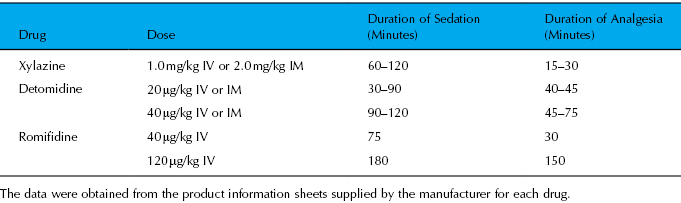
Table 7.2 Duration of sedation and analgesia of alpha-2 adrenergic agonists commonly used in horses
Opioids
Opioids provide moderate to profound analgesia by binding to central and peripheral opioid receptors. Butorphanol is the most commonly used opioid in the horse, but morphine is rapidly gaining in popularity, primarily due to the drug’s long duration of action and minimal cost. Buprenorphine, hydromorphone, and methadone are also used occasionally in horses. Butorphanol is an agonist–antagonist opioid that mediates analgesia through binding to the kappa receptor but not to the mu receptor. Because the most potent analgesia is produced through activation of the mu receptor, butorphanol provides only moderate analgesia. However, because many of the adverse effects associated with opioids may also be mediated more through activation of the mu receptor than activation of the kappa receptor (Clutton 2010), butorphanol may be less likely than the mu opioid agonists (e.g., morphine, hydromorphone, methadone) to cause adverse effects like excitement. However, opioid-mediated excitement in the horse has been somewhat overstated due to misconceptions based on research conducted in nonpainful horses administered opioids at dosages higher than those used clinically. At clinically appropriate dosages, opioids are unlikely to cause significant excitement in horses, especially in horses experiencing pain (Clutton 2010). Furthermore, in horses, the opioids are almost always administered with an alpha-2 agonist, which further decreases the likelihood of excitement. If excitement occurs after the effects of the alpha-2 agonist have dissipated, another dose of alpha-2 agonist or a dose of acepromazine can be used for sedation. Gastrointestinal tract (GIT) adverse effects, like ileus or colic, are also of concern when administering opioids to any species, including horses. However, these effects have also been overstated in horses, and even prolonged dosing may be safe, as horses receiving morphine twice daily for 6 days did not develop abdominal discomfort or colic, although gastrointestinal (GI) transit time was slowed and feces were drier than normal (Boscan et al. 2006). Furthermore, in a study exploring the risk factors that contribute to postoperative colic in the horse, the use of intraoperative morphine was not found to be associated with an increased risk (Andersen et al. 2006). The opioids can be used as boluses, CRIs, or in the epidural space. More information on opioid use in the horse is available in a recently published review article (Clutton 2010).
Local Anesthetic Drugs
Local anesthetic drugs are extremely effective, inexpensive, and easy to use. When local anesthetic drugs are administered, pain impulses originating in the periphery are blocked and prevented from reaching the central nervous system. This blockade has several positive consequences, including rapid and total pain relief from the nerves that are desensitized, allowing many procedures to proceed with minimal dosing of systemic drugs. The blockade also decreases input to the dorsal horn neurons of the central nervous system, thereby decreasing the likelihood of central sensitization and potential amplification or prolongation of the pain sensation.
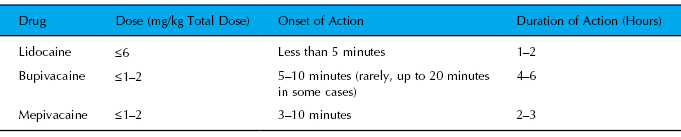
Lidocaine, mepivacaine, and bupivacaine are all used in the horse. Bupivacaine has the longest duration of action of these three local anesthetic drugs and is recommended for any surgery lasting longer than 30–60 minutes. The time to onset of bupivacaine is slightly longer than that of the other drugs (Table 7.3) but generally not long enough to delay the start of most surgical procedures. If immediate onset of action is needed, lidocaine is the drug of choice. Local anesthetics can be used in the skin and underlying tissues at the surgery site, in specific tissues affected by the particular surgery (e.g., in the mesovarian ligament for ovariectomy) and in the epidural space. Also, lidocaine—but not other local anesthetic drugs—can be administered as an IV CRI.
Table 7.3 Dose, time to onset, and duration of action of local anesthetic drugs commonly used in the horse
Acepromazine
Acepromazine provides only mild sedation and no analgesia and is not used alone for sedation of horses presented for standing surgery. However, acepromazine can be used in combination with alpha-2 agonists and opioids to potentiate and prolong sedation. Acepromazine can cause priapism and, although the risk is low (1 in 10,000 horses sedated with acepromazine), most practitioners avoid using the drug in breeding stallions.
Techniques
Initial Sedation
Initial sedation is best achieved with a combination of one of the alpha-2 agonists with one of the opioids, most commonly either morphine or butorphanol. Acepromazine may also be included in the protocol at this stage. Combining the alpha-2 agonist and opioid drug classes provides synergism or additive effects for both sedation and analgesia without an increase in adverse effects (Clarke & Patton 1988; Schatzman et al. 2001; Kruluc & Nemec 2006). The combination also allows lower dosages to be used, which decreases the incidence of dose-related side effects. The alpha-2 agonist should be administered first, and the opioid should be administered after sedation has been achieved (approximately 5–10 minutes after administration of the alpha-2 agonist). If morphine is the opioid of choice, it should be administered IV slowly to prevent potential histamine release and/or excitement. Alternatively, morphine can be administered IM, but the time to onset is prolonged (15–20 minutes).
Prolonging Sedation and Analgesia
Repeat Boluses of Drugs
To achieve sedation and analgesia of adequate duration for the procedure, the alpha-2 agonist and butorphanol can be redosed. Because of long duration of action, neither morphine nor acepromazine requires redosing. Butorphanol is generally redosed only once, even if multiple doses of alpha-2 agonists are required. Depending on the level of sedation of the horse at the time redosing is required and on the projected duration to completion of the procedure, the dose of subsequent boluses of drugs should generally start at 25–50% of the original dose.
CRIs (Table 7.4)
CRIs of sedative and analgesic drugs can provide a more stable plane of sedation and analgesia than that provided by repeat boluses, and the degree of sedation can be easily titrated throughout the entire procedure. The alpha-2 agonist detomidine is the drug most commonly used as a CRI for standing sedation. Boluses of opioids, or a concurrent CRI of opioids, will augment sedation and analgesia. The detomidine CRI is initially administered at a fairly high dose and is then titrated to a lower dose approximately every 15 minutes (Wilson et al. 2002; van Dijk et al. 2003; Goodrich & Ludders 2004). The titration is not critical but will help to prevent excessive sedation and ataxia. If the horse becomes responsive to surgical stimulation, the infusion rate can be increased again. Alternatively, the CRI can be maintained at a low dose constant rate throughout the procedure (Cruz et al. 2004). The CRI is best used with additional analgesia (e.g., epidural or local anesthesia), and supplementation with IV opioids or boluses of detomidine may be necessary (Wilson et al. 2002).
Table 7.4 Analgesic infusions for standing surgery in horses
| Drug(s) | Dosage | Comment, Tip, or Reference |
| Opioids | ||
| Butorphanol | Loading dose: 17.8 µg/kg IV; CRI: 23 µg/kg/h | Quick tip: Add 5 mL of 10 mg/mL butorphanol to 1 L LRS and administer at 1 L/h/450 kg; may need to administer an alpha-2 agonist to prevent possible excitement (Sellon et al. 2004). |
| Alpha-2 agonists | ||
| Detomidine | Loading dose: 8 µg/kg IV CRI: 0.5 µg/kg/min for 15 minutes, followed by 0.3 µg/kg/min for 15 minutes, and finally 0.15 µg/kg/min until 5–15 minutes prior to the end of the procedure | Quick tip: Remove 5 mL of fluid from a 500-mL bag of NaCl and add 5 mL of 10 mg/mL detomidine (for a final concentration of 100 µg/mL of detomidine). Following the loading dose, start the drip (using a 60 drop/mL set) at 0.005 drops/kg/s (roughly 2 drops/s/450 kg) for 15 minutes, then 0.003 drops/kg/s (roughly 1 drop/s/450 kg) for 15 minutes, and then 0.0015 drops/kg/s (roughly 1 drop every other second/450 kg) until 5–15 minutes prior to the end of the procedure (the time between the discontinuance of the drip and the end of the procedure should be based on the degree of sedation and the invasiveness of the procedure). The drip rate should be adjusted to obtain the desired level of sedation. For smaller horses, 2.5 mL of detomidine can be added to the saline to improve the accuracy of counting drops (Goodrich & Ludders 2004). |
| Other drugs | ||
| Lidocaine | Loading dose: 1–1.5 mg/kg IV delivered over 10–20 minutes CRI: 40–50 µg/kg/min | Quick tip: Add 150 mL 2% lidocaine per liter of fluids (generally 750 mL is added to a 5-L bag) and administer the fluids at 1 mL/kg/h for a dose of 50 µg/kg/min; commonly used postoperatively for abdominal pain; could be used intraoperatively for added analgesia during standing surgeries. |
| Ketamine | Loading dose: 0.2–0.6 mg/kg 2–10 µg/kg/min | 0.4–0.8 mg/kg/h (6–13 µg/kg/min) has been used in standing horses (Fielding et al. 2006) and 10 µg/kg/min is commonly used in standing and anesthetized horses. Dosages as low as 2 µg/kg/min seem to be effective in some cases. |
| Combinations (any of the drugs listed in this chart can be used in combination) | ||
| Medetomidine and morphine | See next column | Medetomidine (5 µg/kg IV) followed in 10 minutes by morphine (50 µg/kg IV) and 10 minutes later by a CRI of medetomidine and morphine (5 and 30 µg/kg/h, respectively; Solano et al. 2009) |
Opioid CRIs are also used for standing procedures. Butorphanol has been used alone for postoperative pain (Sellon et al. 2004) but is generally used with an alpha-2 agonist for standing surgical procedures (Goodrich & Ludders 2004). Morphine is used with an alpha-2 agonist and has been shown to provide “reliable sedation” without excitement and stable cardiorespiratory function in horses undergoing standing laparoscopy (Solano et al. 2009). The opioid can be combined in the bag or syringe with the alpha-2 agonist but is generally administered separately, allowing more flexibility to change the rate of the alpha-2 agonist CRI without affecting the delivery of the opioid. Lidocaine and ketamine are often used as analgesic CRIs in both conscious and anesthetized horses, and either CRI could be used to supplement analgesia in standing surgical procedures. More information on these CRIs is available in the chapter on general anesthesia and in two recently published review articles (Doherty & Seddighi 2010; Muir 2010).
Local Blockade
Local anesthetic drugs should be used in all standing surgeries. Several options are available for local anesthetic blockade, including local desensitization of the incision site, regional desensitization of the surgical area, and desensitization of the structures involved in the specific surgery. Frequently, the portal sites are infiltrated directly with lidocaine, mepivacaine, or bupivacaine (Hendrickson 2006). If an incision is required for the removal of tissue like ovaries or testicles, the incision site can also be directly infiltrated. To desensitize all of these sites, 10–30 mL of local anesthetic drug is commonly utilized. Even with volumes this large, the dose is still far below the maximum clinically used dose of 4–6 mg/kg lidocaine or 1–2 mg/kg bupivacaine. Desensitization of the entire lumbar fossa can be achieved using techniques similar to those used in cattle for standing abdominal surgery. Proximal and distal paravertebral regional blockades, although not commonly used, have been described in the horse (Moon & Suter 1993; Röcken et al. 2007). An “inverted L” regional blockade has also been used (Hendrickson & Wilson 1997). Finally, desensitization of discrete structures involved in specific surgeries should be used. For instance, the mesorchium or the mesovarium can be injected with local anesthetics for testicle or ovary removal, respectively (Hendrickson 2006). For castration, blockade of either the testicle or the mesorchium provided equal analgesia (Joyce & Hendrickson 2006). For ovariectomy, mesovarian blockade provided better analgesia than intraovarian blockade (Farstvedt & Hendrickson 2005). Although local anesthetic blockade occurs fairly quickly, when local anesthetic drugs require absorption from a large area like the mesorchium, testicle, mesovarium, or ovary, a 15-minute lag time between local anesthetic injection and commencement of surgery will increase the likelihood that full blockade has occurred. Full blockade can have a major impact on the success of the surgery as “incomplete anesthesia of the testis or mesorchium can lead to excess movement” and “desensitization of the ovarian pedicle with local anesthetic will reduce movement of the horse, making the surgery easier to perform” (Hendrickson 2008).
Examples of other uses of local anesthetic blockade during laparoscopy include retroperitoneal infiltration of local anesthesia for nephrectomy (Keoughan et al. 2003; Cokelaere et al. 2007), local infiltration of the intestine at biopsy sites (Bracamonte et al. 2008), and lidocaine-soaked gauze in the vaginal vault for transvaginal laparoscopy (Alford & Hanson 2010).
Epidural Analgesia (Figure 7.1)
Analgesia of the hind limbs and caudal abdomen can be achieved by injecting drugs into the epidural space. Systemic sedation will also be necessary, but the dose of sedative drugs can generally be reduced when epidural analgesia is provided. The most commonly used drug in the epidural space is morphine, which provides analgesia of long duration (approximately 12 hours) with minimal to no systemic effects and no motor dysfunction. Dilution of the morphine (0.1 mg/kg) with 10–30 mL of sterile saline or sterile water (in an adult horse) will insure cranial migration of the drug to a level of the spinal cord that is in proximity to the surgery site. The time to onset of analgesia when morphine is delivered in the epidural space is 30–45 minutes, necessitating additional analgesia for the beginning of the surgical procedure. Epidural morphine provided effective analgesia, improved patient comfort, and reduced the sedation needed to perform ovariectomy (Van Hoogmoed & Galuppo 2005). Alpha-2 agonists, especially detomidine, are also commonly used in the epidural space. Detomidine is the alpha-2 agonist most commonly used, and a dose of 40 µg/kg diluted with sterile water or sterile saline to a total volume of 12–15 mL per adult horse is standard (Hendrickson 2008). A dose of 60 µg/kg has also been reported but may result in excessive sedation and possible ataxia secondary to systemic absorption (Hendrickson 2008). Although analgesia provided by a detomidine CRI appears to be equal to analgesia provided by a detomidine epidural, the epidural may have a slight advantage in that it provided analgesia during initial manipulation of the ovary but the CRI did not (Virgin et al. 2010). A combination of detomidine and morphine may be more effective and longer lasting than either drug used alone (Sysel et al. 1996; Goodrich et al. 2002). Local anesthetic drugs are rapidly effective in the epidural space (3–5 minutes) but indiscriminately desensitize both sensory and motor nerves, resulting in ataxia if the drug reaches the motor nerves controlling rear limb function. Thus, the local anesthetics are commonly used for procedures involving the perineum but are rarely used for more cranial procedures. The site of injection for epidurals in horses is generally the sacrococcygeal vertebral body junction or the junction between coccygeal vertebral bodies 1 and 2 or 2 and 3, but lumbosacral injections have been used. Finally, long-duration analgesia can be provided by placing an indwelling epidural catheter and delivering repeat boluses of morphine every 12 hours (Sysel et al. 1997). A review of epidural analgesia in the horse has been published (Natalini 2010).
Figure 7.1 Epidural injections of opioids and/or alpha-2 agonists are often used to provide analgesia for laparoscopic surgery. If the surgery will be prolonged or if the pain following the surgery will be prolonged, repeat epidural injections may be necessary. Conversely, placement of an epidural catheter will facilitate repeat administrations of analgesic drugs without the need for repeat needle punctures for the horse. Catheters are most commonly placed in the sacrococcygeal or first coccygeal junctions but can also be placed in the lumbosacral space, as in these photographs. (A) Components of an epidural catheter kit—components of a typical catheter kit including the spinal needle, which serves as a guide needle for the catheter, the catheter itself (coiled in a sterile bag at top left), and a bacterial filter to place at the end of the catheter. (B) Insertion of epidural needle—the epidural guide needle is inserted into the epidural space. (C) Catheter insertion into spinal needle—the epidural catheter is inserted through the epidural guide needle into the epidural space. The needle will then be removed and the catheter will be capped with the bacterial filter. (D) Securing and covering the catheter—final preparation of the catheter site includes securing the catheter with suture and covering the catheter with sterile adhesive dressing.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


