The first instrument portal is established by placing a 10- to 12-mm cannula using a blunt obturator through a 1-cm skin incision approximately 25 cm cranial to the umbilicus and 15 cm left of the ventral midline. A 25-cm skin incision is made starting 5 cm caudal to the first instrument portal and extending parallel to the ventral midline in a caudal direction. A second instrument cannula is placed 5 cm caudal and 2 cm axial to the long skin incision. A third instrument cannula is placed 8 cm axial to the second. The original description of laparoscopic colopexy (Trostle et al. 1998) had instrument portals axial and abaxial to the caudal limit of the skin incision; however, in some horses, the left thigh of the horse compromised needle holder manipulation.
The left ventral colon is identified and the lateral taenia of the left ventral colon is grasped with an endoscopic Babcock forceps placed through the cranial instrument portal, and the colon is elevated toward the ventral body wall (Figure 24.2). The suture material chosen for the colopexy would preferably be a monofilament with a relatively long-term retention. The author uses size 1 polyglyconate (Maxon, Tyco Healthcare, Norwalk, CT) in a 60-in. strand with a large half-curved needle. After fashioning the needle into a ski-tip configuration, the needle is placed through the abdominal wall at the cranial extent of the large skin incision. The needle is grasped within the abdomen with a needle holder placed through the most abaxial caudally placed cannula. A correct grasp of the needle is facilitated by rotating the needle from outside the abdomen (Figure 24.3). A bite of the taenia is taken and, using an instrument placed through the axial caudal cannula (Figure 24.4), the needle is repositioned in the needle holder and passed out of the abdomen. After the first suture placement, the needle can be placed through the taenia without using the Babcock forceps. The author routinely places a spinal needle through the abdominal wall to give perspective as to where the suture should exit (Figure 24.5). The colon is pulled into contact with the abdominal wall and tied, establishing the cranial end of a continuous suture. The process of suture placement is continued until a 20-cm pexy has been established (Figure 24.6) and the suture is tied off outside the abdomen. The abdomen is deflated and incision closures are routine.
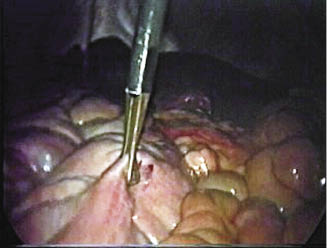
Figure 24.2 Intra-abdominal cranial viewing image demonstrating an endolaparoscopic Babcock grasping forceps the lateral taenia on the left ventral colon.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


