It is convenient to store all the necessary nonsterile components of the equipment arsenal on a portable cart, sometimes called the video tower, as pictured in Figure 5.2.
Figure 5.2 Video tower (from top to bottom): monitor, image capture system, insufflator, light source, camera control unit, and printer.
Source: KARL STORZ GmbH & Co. KG.

Telescopes and Instruments
Laparoscopes
The telescope or laparoscope is analogous to a large version of an arthroscope. It consists of a series of high quality optical glass rod lenses placed at specific distances within a stainless steel tube, along with thousands of glass fibers that transmit light to the tip of the telescope to illuminate the subject. The light is delivered from a remote light source that is connected via a fiber-optic cable to the light guide post of the telescope. While the operator can look directly into the eyepiece of the telescope, more commonly, this is where the head of an endoscopic video camera is attached for transmission of the image to a large viewing monitor.
Standard laparoscopes made for minimally invasive surgery in people are typically 10 mm in diameter and approximately 33 cm in length. For applications in large animals, some manufacturers make extended length telescopes between 50 and 60 cm in length (see Figure 5.3). The latter is useful for performing certain procedures through a single port, such as a thorough examination of the entire abdomen or a bilateral cryptorchidectomy. Sometimes, however, the shorter telescopes are more convenient for surgeries such as ovariectomy, where the added length is neither necessary nor convenient.
Figure 5.3 Equine laparoscope, 10-mm diameter × 57-cm working length.
Source: KARL STORZ GmbH & Co. KG.

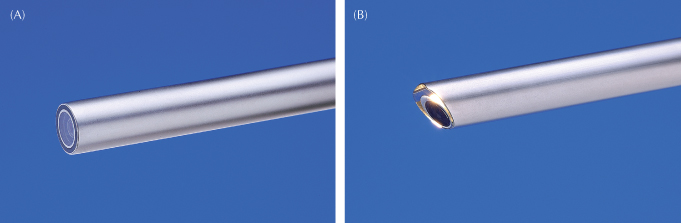
The tip of the telescope may be forward viewing or angled, as shown in Figure 5.4. The angled view enables the operator to see a larger field of view by rotating the telescope along its longitudinal axis; however, hand–eye coordination during surgery is a bit more challenging when using an angled telescope.
Figure 5.4 Telescope tips: (A) forward viewing or 0° versus (B) forward oblique or 30°.
Source: KARL STORZ GmbH & Co. KG.
An operating laparoscope like the one pictured in Figure 5.5 contains an integral operating channel. With this type of telescope, 5-mm instruments can be passed into the abdomen under visualization through a single portal. The eyepiece is offset to avoid interference with the instrumentation and the hands of the clinician.
Figure 5.5 Operating laparoscope, 10-mm outer diameter with 6-mm integral channel for the passage of 5-mm instruments.
Source: KARL STORZ GmbH & Co. KG.

Laparoscopes should be handled with care and stored in a protective case away from other instruments as any shock insult to the scope could crack or dislodge a rod lens, resulting in an unclear image.
Trocars and Cannulas
The insertion of the laparoscope and instruments into the abdomen requires portals or cannulas that ideally meet the following criteria:
- Safe and easy placement and removal
- Remain in place and maintain pneumoperitoneum during surgery
- Easily cleaned and sterilized (or replaced)
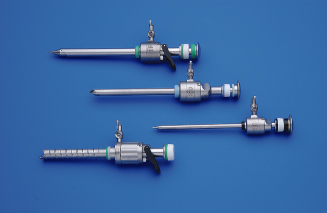
A variety of laparoscopy trocars are pictured in Figure 5.6. A conventional trocar includes a cannula that will provide the portal for instruments and telescopes, as well as a sharp or blunt-tipped trocar that is used to penetrate the abdominal wall initially and is then removed from the cannula. The terminology can be somewhat confusing as the term trocar may refer to the obturator alone or the combination of trocar (obturator) and cannula together.
Figure 5.6 Reusable laparoscopy trocars come in many styles and sizes.
Source: KARL STORZ GmbH & Co. KG.
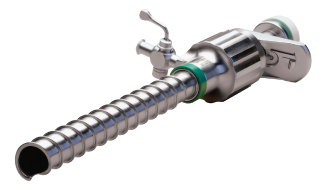
Laparoscopic cannulas contain a one-way valve that permits the insertion of instruments, but snaps shut when the instrument is removed, so that pneumoperitoneum is maintained. Multifunctional valves such as those in Figure 5.7 can be manually opened during a procedure by pressing the black lever. This is convenient to rapidly release insufflation gas or to prevent dulling of sharp instruments or needles upon insertion.
Figure 5.7 Equine trocars with multifunctional valves, 20-cm working length, 6 mm (top) and 11 mm (bottom).
Source: KARL STORZ GmbH & Co. KG.

Many cannulas also include a lateral Luer lock connector to which the insufflation tubing can be connected.
Trocars come in a variety of diameters and lengths. Since most laparoscopic instruments are either 5 or 10 mm in diameter, the corresponding cannula sizes 6 and 11 mm are the most popular. The inner diameter of a cannula is slightly larger than the outer diameter of the instruments or telescopes designed to pass through it so that insufflation gases can flow freely around the instrument to maintain pneumoperitoneum during surgery. Sometimes, larger cannulas, up to 25 mm in diameter, are used to extract large masses or to introduce larger instrumentation such as staplers or ultrasound probes.
Reducers permit the use of 5-mm instruments through 10-mm cannulas. The reducer in Figure 5.8 attaches to the neck of the cannula and the cap is flipped into the hole of the larger diameter rubber washer on the 10-mm cannula, reducing its diameter to avoid the escape of gas when a 5-mm instrument is inserted.
Figure 5.8 Laparoscopy trocar (11 mm) with a reducer that allows the passage of 5-mm instruments, without leakage of insufflation gas.
Source: KARL STORZ GmbH & Co. KG.

While standard laparoscopy trocars designed for human surgery tend to be 10 cm long or shorter, some manufacturers produce 20-cm trocars like those in Figure 5.7, which are much more convenient for standing procedures in the horse.
Many equine surgeons prefer to avoid the use of a sharp-tipped trocar for the initial puncture as this must be done blindly—before the telescope is inserted—and could therefore inadvertently cause trauma to intra-abdominal viscera. The second and third punctures can be executed safely with a sharp-tipped trocar under the direct visualization of the laparoscope.
Depending on the positioning of the patient, technique of insufflation, and operator preference, there are several options for an atraumatic placement of the first trocar, as described in the technique chapters of this text. One such technique is called the Hasson technique, which employs a blunt-tipped trocar and requires a surgical placement, thus avoiding the forceful insertion of a sharp trocar. Another involves the use of an EndoTIP® trocar, pictured in Figure 5.9. This type of trocar is inserted through a body wall stab incision with a twisting motion and can be guided visually with the telescope in place as the layers of muscle and fascia are traversed. Rather than cutting the tissues, this type of trocar separates or displaces the tissues such that the integrity of the fasciae is mostly preserved, resulting in a less traumatic trocar entry that may also reduce the risk of postoperative hernias. Note that it is most effective to insufflate prior to the placement of an EndoTIP® trocar so that the peritoneum is taut and less likely to move away from the trocar upon insertion.
Figure 5.9 An EndoTIP® cannula is inserted through a stab incision in the body wall with a twisting motion. The surgeon can visually monitor entry with the telescope in the cannula during insertion.
Source: KARL STORZ GmbH & Co. KG.
Information on bladeless/guarded trocars, which are mostly manufactured as disposable or single-use instruments, can be found in Chapter 6.
Hand Instruments
A vast array of hand instruments is available for laparoscopic surgery in a variety of lengths and diameters. As for the telescopes and trocars, extended length versions of at least 40 cm are convenient, and in some cases essential, for equine laparoscopy. The 10-mm diameter instruments tend to be more robust than standard 5-mm instruments and are therefore more popular for use in equids, when available. The most commonly used hand instruments for equine laparoscopy include grasping forceps (both traumatic and atraumatic), scissors, dissecting forceps, and any of several options for ligation.
Two styles of atraumatic graspers are shown in Figure 5.10. The 10-mm diameter, 43-cm shaft and long jaws make these instruments ideal for gently manipulating equine viscera. Note that the handles contain a swing-away ratchet, which enables the surgeon to use the instrument with or without a ratchet handle as desired. Also note that the lower instrument has an insulated handle and connecting pin for a monopolar electrosurgical cable. Many different handle styles are available, and may be interchangeable, depending upon the manufacturer’s design.
Figure 5.10 Atraumatic grasping forceps, 10-mm diameter × 43-cm working length.
Source: KARL STORZ GmbH & Co. KG.

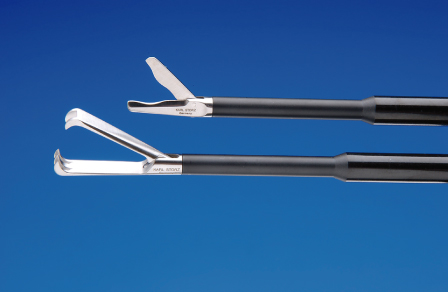
Two other commonly used 10-mm instruments shown in Figure 5.11 are a pair of robust tissue scissors and traumatic grasping forceps, used only for grasping tissue that will be removed, such as ovaries and testes during ovariectomy and cryptorchidectomy.
Figure 5.11 Equine laparoscopic scissors and traumatic grasping forceps, 10-mm diameter × 43-cm working length.
Source: KARL STORZ GmbH & Co. KG.
Dissecting forceps are available with many different jaw types. The most popular among equine styles for equine laparoscopy are curved Kelly forceps and right-angle dissectors (Figure 5.12).
Figure 5.12 Atraumatic grasping forceps jaws: curved Kelly (A) and right-angle graspers (B).
Source: KARL STORZ GmbH & Co. KG.

Ligation of tissues and bleeders can be achieved by many means, including the following:
- Loop ligatures (Figure 5.13)
- Bipolar forceps, useful for grasping and coagulating (Figure 5.14)
- “Tripolar” forceps enable grasping, coagulating, and transecting with a single bipolar instrument; after grasping and coagulating with the jaws, a cutting blade is advanced between the two sets of grasping jaws (Figure 5.15)
- Needle holders for intracorporeal suturing and knot tying (Figure 5.16)
- Knot pushers, for sliding extracorporeal knots down to the surgical site (Figure 5.17)
- Clip appliers (Figure 5.18; see Chapter 6)
- Staplers (see Chapter 6)
- Vessel-sealing and dividing devices (see Chapter 6)
Figure 5.13 A pretied loop ligature.
Source: KARL STORZ GmbH & Co. KG.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


