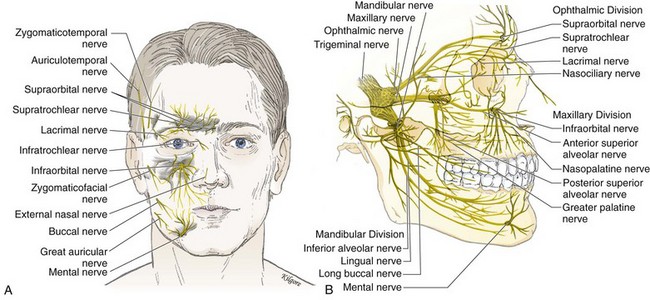
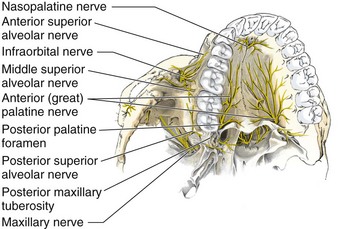
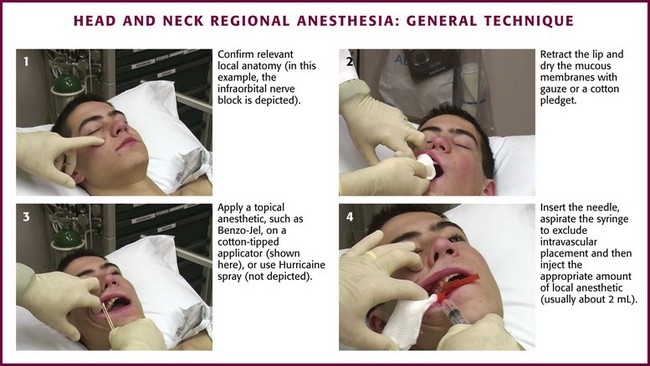
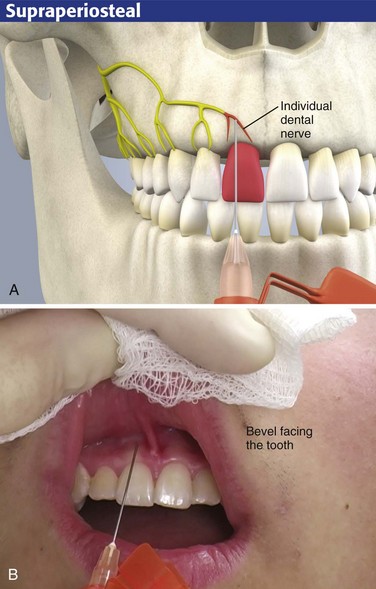
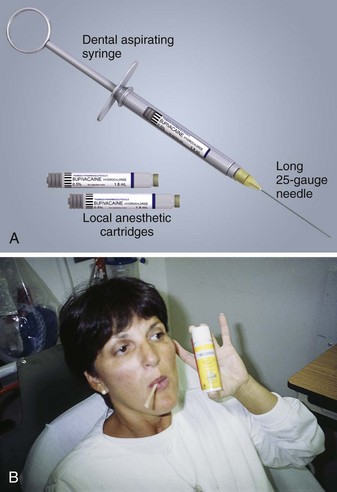
Chapter 30 Intraoral and extraoral regional anesthesia is simple and convenient for everyday use in the emergency department (ED).1 Nerve blocks provide anesthesia to broad areas of distribution on the face with a minimal amount of anesthetic and tissue distortion. Local anesthetic blocks are effective for closing facial lacerations, especially those of the lips, forehead, midface, and ears, places where the swelling caused by local infiltration may be undesirable. Local anesthetic blocks are also effective for the relief of pain, for anesthesia during facial débridement, and for diagnostic purposes. Regional blocks are also therapeutic for procedural anesthesia and for control of pain in dental emergencies such as toothaches and dry sockets (see Chapter 64). Patients with dental pain who do not obtain relief with a regional dental block most likely do not have pain of dental origin. In cases in which the patient is thought to be seeking drugs, a dental anesthetic block is frequently the treatment of choice as an alternative to narcotics. Topical anesthetic solutions such as tetracaine-adrenaline-cocaine (TAC) solution are useful for small lacerations of the scalp and face because of the vascularity of these areas. TAC is not to be used on or near the mucous membranes or the eye (see Chapter 29). More extensive discussion of the general complications of local anesthetics and regional anesthesia is provided in Chapters 29 and 32, respectively. Ophthalmologic anesthesia is discussed in Chapter 62, and blocks about the ears and nasal anesthesia are discussed in Chapter 63. The fifth cranial nerve, known as the trigeminal nerve, is the sensory nerve to the face (Fig. 30-1A) and the largest of the cranial nerves. It takes its origin from the midbrain and enlarges into the gasserian, or semilunar, ganglion. Each gasserian ganglion supplies one side of the face. The gasserian ganglion is a flat, crescent-shaped structure approximately 10 mm long and 20 mm wide that divides into three branches: the ophthalmic, maxillary, and mandibular nerves (Fig. 30-1B). 1. The medial and lateral branches of the supraorbital nerve, which emerge on the face through the supraorbital notch. These two sensory nerves pierce the frontalis muscle and extend to the lambdoid suture on the back of the skull. 2. The supratrochlear nerve, which provides sensation to the medial aspect of the forehead just above the glabella. Branches of the ophthalmic nerve provide sensation to the forehead, cornea, upper eyelid, structures in the orbit, and the frontal sinuses. The anatomy of the maxillary nerve is rather complicated because of its numerous branches. The first branch comprises two short sphenopalatine nerves to the pterygopalatine ganglion, also called the Meckel ganglion or the sphenopalatine ganglion. The next two branches of clinical importance are the nasopalatine and the greater (anterior) palatine nerves. The nasopalatine nerve arises from the pterygopalatine ganglion, courses down along the nasal septum, and is transmitted through the anterior portion of the hard palate by way of the anterior palatine canal. This canal is located in the midline approximately 10 mm palatal to the maxillary central teeth and immediately behind the incisors. The nasopalatine nerve provides sensation to the most anterior portion of the hard palate and the adjacent gum margins of the upper incisors. This nerve is rarely blocked in clinical practice, except in dental operations, because it is quite painful as a result of the tightly bound tissues (Fig. 30-2). The anterior, or greater, palatine nerve arises from the pterygopalatine ganglion and passes down through the posterior palatine foramen. The posterior palatine foramen is located 10 mm palatal to the third molar and the bicuspid teeth and intermingles with the nasopalatine nerve opposite the cuspid tooth. The greater palatine nerve provides sensation to most of the hard palate, as well as the palatal aspect of the gingiva. It is rarely blocked in the ED (see Fig. 30-2). The next branch consists of the posterior superior alveolar (PSA) nerve, which courses down the posterior surface of the maxilla for approximately 20 mm, at which point it enters one or several small posterosuperior dental foramina (see Fig. 30-2). This nerve supplies all the roots of the third and second molar teeth and two roots of the first molar tooth. A third branch consists of the middle superior alveolar (MSA) nerve, which branches off about midway within the infraorbital canal and then courses downward in the outer wall of the maxillary sinus (see Fig. 30-2). This nerve supplies the maxillary first and second bicuspid teeth and the mesiobuccal root of the first molar. The last branch consists of the anterior superior alveolar (ASA) nerve, which branches off into the infraorbital canal approximately 5 mm behind the infraorbital foramen, just before the terminal branches of the infraorbital nerve emerge (Fig. 30-2). This nerve descends in the anterior wall of the maxilla to supply the maxillary central, lateral, and cuspid teeth; the labial mucous membrane; the periosteum; and the alveoli on one side of the median line. There is intercommunication among the ASA, MSA, and PSA nerves. 1. The long buccal nerve branches off just outside the foramen ovale. It passes between the two heads of the external pterygoid muscle and crosses in front of the ramus to enter the cheek through the buccinator muscle, buccal to the maxillary third molar. The buccal nerve supplies sensory branches to the buccal mucous membrane and the mucoperiosteum over the maxillary and mandibular teeth. The cutaneous branch provides sensation to the cheek. 2. The lingual nerve courses forward toward the midline. It runs downward superficially to the internal pterygoid muscle and passes lingual to the apex of the mandibular third molar. It enters the base of the tongue at this point through the floor of the mouth and supplies the anterior two thirds of the tongue, the lingual mucous membrane, and the mucoperiosteum. 3. The largest of the V3 branches is the inferior alveolar nerve. It provides sensation to all the lower teeth, although the central incisors, lateral incisors, and buccal aspect of the molar teeth may receive additional sensory innervation. The nerve descends, covered by the external pterygoid muscle, and passes between the ramus of the mandible and the sphenomandibular ligament to enter the mandibular canal. It is accompanied by the inferior alveolar artery and vein, proceeds along the mandibular canal, and innervates the teeth. At the mental foramen the nerve bifurcates into an incisive branch, which continues forward to supply the anterior teeth. It gives off a side branch, the mental nerve, which exits from the mental foramen to supply the skin. The mental foramen is located approximately between the apices of the lower first and second bicuspids, or premolar teeth. This is a useful site at which to perform a nerve block because the mental nerve provides sensation to the skin of the chin and the mucous membrane of the lower lip. Extraoral injections can be done easily with a 3-mL Luer-Lok syringe and a Figure 30-3 A, Local anesthesia—basic setup for intraoral application using an aspirating dental syringe. B, Topical mucosal anesthesia can make the injection nearly painless. Swab the gauze-dried mucosa with the topical agent or have the patient hold cotton swabs soaked in the agent, and wait for 1 to 3 minutes. Benzocaine can be used as a topical anesthetic (shown here). However, excellent topical anesthesia of mucous membranes can be obtained after 2 minutes by applying a gel mixture of a topical anesthetic consisting of 10% lidocaine, 10% prilocaine, and 4% tetracaine. (Profound, Steven’s Pharmacy, Costa Mesa, CA. Available at www.stevensrx.com). Use needles no smaller than 27 gauge for block techniques because a higher-gauge needle makes aspiration difficult and can thus result in inadvertent intravascular injection. Intravascular epinephrine, though used in small doses, may produce systemic symptoms (anxiety, tachycardia), as well as painful vasospasm if injected intraarterially, but the amount of local anesthetic is generally inconsequential.2 Most patients fear dental blocks greatly, and the anxiety and pain may be lessened considerably with the use of topical anesthetics applied to the mucous membranes before injection (Fig 30-4, step 3). It is important to dry the injection site thoroughly with gauze before the injection (see Fig 30-4, step 2) because copious saliva will wash the anesthetic away prematurely. Coat a cotton-tipped applicator generously with 20% benzocaine (Hurricaine, Beutlich, Inc., Niles, IL) or 5% to 10% lidocaine so that the area of injection is completely covered. Allow the patient to hold the cotton swab in place. The area will be anesthetized in 2 to 3 minutes. Use concentrated topical anesthetics because poor results are obtained with weaker preparations such as 2% viscous lidocaine. Cocaine (4%) is another acceptable topical anesthetic. The most common technique for intraoral local anesthesia of individual teeth is supraperiosteal infiltration (Fig. 30-5). This technique can provide complete relief of a toothache. Select the area to be anesthetized and dry it with gauze. Apply a topical anesthetic, such as 20% benzocaine or 5% lidocaine ointment, as described. Ask the patient to close the jaw slightly and relax the facial musculature. Grasp the mucous membrane of the area with a piece of gauze. Pull the gauze outward and downward in the maxilla and outward and upward in the mandible to extend the mucosa fully and to delineate the mucobuccal fold. Puncture the mucobuccal fold with the bevel of the needle facing the tooth. Aspirate the area and deposit approximately 1 to 2 mL of local anesthetic (2% lidocaine should be used here) at the apex (area of the root tip) of the involved tooth (see Fig. 30-5). It is helpful to place a finger against the outer aspect of the lip overlying the injection site. Apply firm and steady pressure against the lip and slowly inject the local anesthetic into the supraperiosteal site. This helps prevent ballooning of the lip.
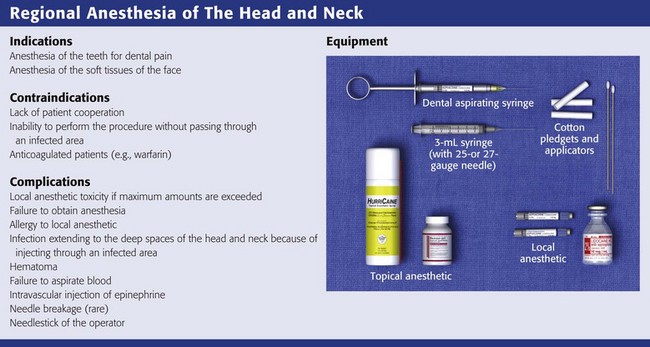
Regional Anesthesia of the Head and Neck
Anatomy of the Fifth Cranial (Trigeminal) Nerve
Ophthalmic Nerve
Maxillary Nerve
Mandibular Nerve
Equipment for Dental and Cranial Nerve Blocks
 -inch, 25- to 27-gauge needle. A needle no smaller than 27 gauge is recommended for deep block techniques because of the inability to perform aspiration. Generally, a long needle is used for nerve blocks and a short needle is used for infiltration. Intraoral local anesthesia can also be conveniently administered with a dental aspirating syringe, which uses a Carpule cartridge of anesthetic along with a disposable needle (Fig. 30-3A). Dental aspirating syringes are not mandatory for intraoral local anesthesia but they make the procedure simpler, particularly when aspirating. Other adjuncts that are helpful in the administration of intraoral anesthesia include topical mucosal anesthetic agents such as gels or sprays because they can make the injection nearly painless (Fig. 30-3B). First swab the gauze-dried mucosa with a topical agent or have the patient hold cotton swabs soaked in the agent to the anticipated injection site, and wait for 1 to 3 minutes. Excellent topical anesthesia of the mucous membranes can be achieved after 2 minutes by applying a gel mixture of a topical anesthetic consisting of 10% lidocaine, 10% prilocaine and 4% tetracaine (Profound, Steven’s Pharmacy, Costa Mesa, CA; www.stevensrx.com).
-inch, 25- to 27-gauge needle. A needle no smaller than 27 gauge is recommended for deep block techniques because of the inability to perform aspiration. Generally, a long needle is used for nerve blocks and a short needle is used for infiltration. Intraoral local anesthesia can also be conveniently administered with a dental aspirating syringe, which uses a Carpule cartridge of anesthetic along with a disposable needle (Fig. 30-3A). Dental aspirating syringes are not mandatory for intraoral local anesthesia but they make the procedure simpler, particularly when aspirating. Other adjuncts that are helpful in the administration of intraoral anesthesia include topical mucosal anesthetic agents such as gels or sprays because they can make the injection nearly painless (Fig. 30-3B). First swab the gauze-dried mucosa with a topical agent or have the patient hold cotton swabs soaked in the agent to the anticipated injection site, and wait for 1 to 3 minutes. Excellent topical anesthesia of the mucous membranes can be achieved after 2 minutes by applying a gel mixture of a topical anesthetic consisting of 10% lidocaine, 10% prilocaine and 4% tetracaine (Profound, Steven’s Pharmacy, Costa Mesa, CA; www.stevensrx.com).
General Recommendations
Technique
Supraperiosteal Infiltration
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Regional Anesthesia of the Head and Neck