Alison B. Clode
Recurrent Uveitis
Equine recurrent uveitis (ERU), colloquially known as moon blindness or periodic ophthalmia, is a syndrome of panuveitis (anterior and posterior segment inflammation) that entails bouts of inflammation followed by periods of quiescence. Establishing chronicity and recurrence, which occur with variable frequency and intensity in individual horses, is essential for diagnosing a horse with ERU because not all uveitis may be characterized as recurrent. Specifically, a horse experiencing an initial episode of primary uveitis, such as might be caused by a traumatic episode or an infection that resolves with appropriate treatment and does not recur in subsequent months to a few years, does not have ERU. In horses in which ERU is ultimately diagnosed, it is suspected that the initial bout of inflammation compromises the immune-privileged ocular environment, allowing lymphocyte infiltration into the uveal tract, which is normally devoid of these cells. These lymphocytes, predominantly CD4+ T cells, secrete proinflammatory cytokines such as interleukin-2 (IL-2) and interferon-γ (IFN-γ) and are primed to initiate the inflammatory process when reexposed to inciting antigens. In ERU, immunologic mechanisms implicated in initiating recurrence include molecular mimicry, bystander activation, and epitope spreading. These mechanisms enable the primed immune cells to respond to similar, but not identical, epitopes that may arise from known-antigenic ocular locations (such as the retina) rather than from the specific initial inciting antigen. This underlying immune-mediated mechanism for ERU is the basis for treatment with immunosuppressive medications.
In some instances, the spirochete bacterium Leptospira interrogans (specifically serovars Pomona and Grippotyphosa) has been implicated in initiating ERU. Following initial exposure, generally through contact with groundwater contaminated with urine from reservoir animals (deer, cattle, swine, and rats), most horses develop mild, self-limited signs of infection, such as fever, anemia, and inappetence, generally with minimal ocular inflammation. As with other causes of uveitis, loss of ocular immune privilege ensues, and activated immune cells become sequestered in the uveal tract, potentially along with L interrogans antigens, thus perpetuating inflammatory episodes. An additional unique immunologic aspect of leptospiral infection is cross-reactivity between L interrogans antibodies and ocular tissues (e.g., the tear film, cornea, lens, aqueous humor, ciliary body, and retina). These antigenic similarities allow primed immune cells within the eye to be stimulated by exposure to these ocular tissues, again through the processes of molecular mimicry, bystander activation, and epitope spreading. Appaloosas with a serologic titer of antileptospiral antibodies have the poorest prognosis for vision, and conversely, non-Appaloosa horses with negative serology have the best prognosis for vision. Geographic variability in the role of L interrogans has been suggested, with as many as 79% of European horses with ERU having aqueous humor (AH) or vitreous humor (VH) titers, compared with horses in the United States, in which no such correlation has been demonstrated.
Classification
The classification scheme for ERU includes the classic recurrent, insidious, and posterior forms. Horses with the classic recurrent form experience active, outwardly identifiable clinical signs of anterior uveitis, followed by a response to therapy and temporary resolution of clinical signs, whereas the insidious form manifests as low-grade, continual anterior (and frequently posterior) uveitis, in the absence of clinical signs recognizable without detailed ophthalmic examination. Posterior uveitis does not produce anterior uveitis, but rather produces inflammation of the retina, choroid, and vitreous. Insidious ERU is most common in the Appaloosa and in draft breeds, whereas posterior uveitis is most common in warmbloods, draft breeds, and European horses.
Clinical Signs and Diagnosis
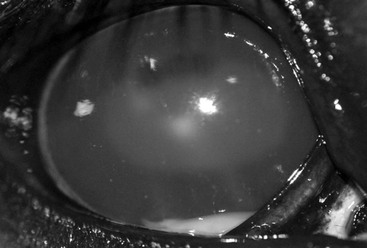
The clinical signs of ERU vary considerably, depending on the form, preexisting ocular changes, chronicity, and response to treatment. Horses with active anterior uveitis develop varying degrees of blepharospasm, blepharedema, and epiphora, with flare, hypopyon, or hyphema, miosis, and ocular hypotony (intraocular pressure [IOP] <10 mm Hg) consistently present (Figure 150-1). Additionally, keratic precipitates (accumulations of cells and inflammatory debris on the corneal endothelium), synechia formation, resistance to mydriasis, and iridal color changes may be seen. Signs developing with chronicity include iridal hyperpigmentation, corpora nigra atrophy, cataract, permanent synechiae, ocular hypertension (IOP >30 mm Hg) secondary to pupillary occlusion and subsequent obstruction of aqueous humor flow, or phthisis bulbi (Figure 150-2). Corneal involvement (manifested as mild edema, lackluster haziness, perilimbal superficial vascularization, or calcific band keratopathy) may be observed with both active and chronic inactive ERU, but it must be distinguished from a primary corneal disease process, which generally manifests with more significant edema, vascularization, and corneal cellular infiltrate. Horses with posterior uveitis may develop vitritis, identified as a yellowish appearance, liquefaction, and cellular infiltration of the vitreous, with or without fibrous traction bands, all of which may be significant enough to obscure the fundus (Figure 150-3). Chorioretinitis manifests as depigmented and hyperpigmented lesions surrounding the optic disc (“bullet-hole” or “butterfly” lesions) or as retinal detachment. Classic recurrent and posterior ERU are more likely to be unilateral, whereas insidious ERU is more commonly a bilateral (although not necessarily symmetric) disease.

< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


