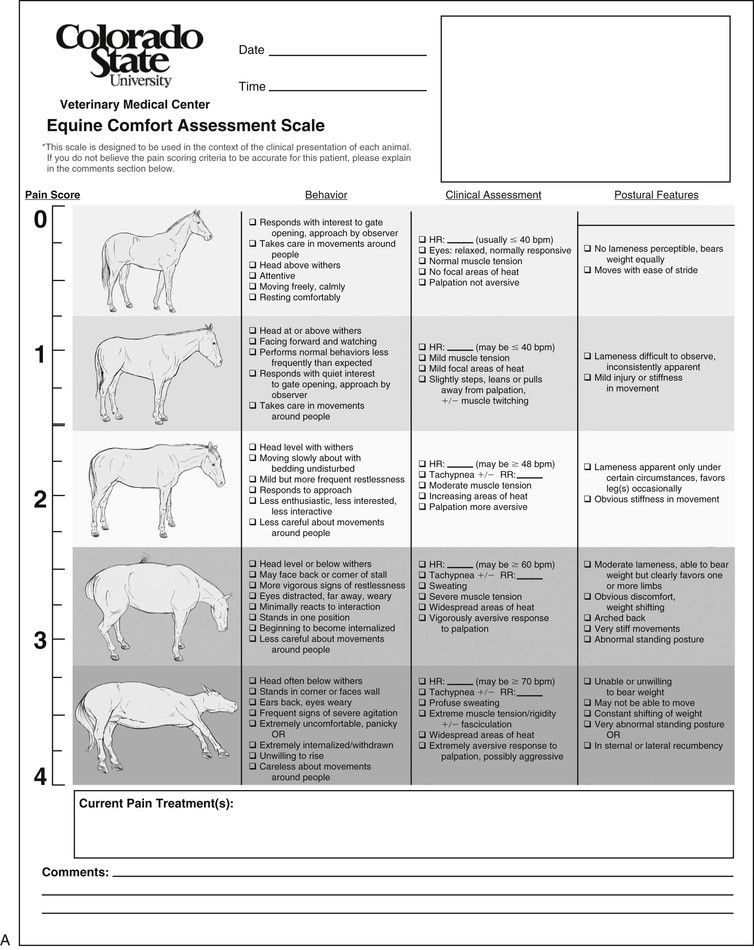
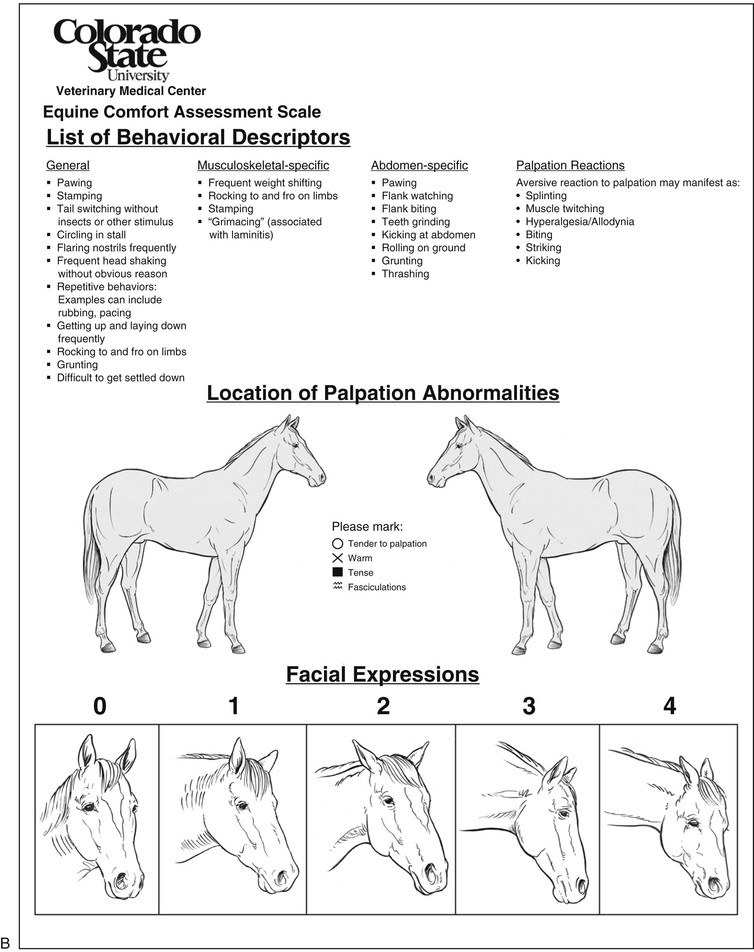
Erin K. Contino, Khursheed R. Mama Pain is defined by the International Association for the Study of Pain as an “unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.” Because the horse cannot verbally describe the impact of this unpleasant experience, and because situational factors such as sedation or paralysis may preclude a horse’s ability to express pain, it falls upon the observer to identify and quantify pain in horses. Unfortunately, despite efforts in the past decade to develop reliable and objective pain scales, assessing pain in horses remains challenging and is confounded by the many different manifestations and types of pain. For example, pain can be described by mechanism (e.g., nociceptive, neuropathic, or inflammatory), location (somatic or visceral), duration (acute or chronic), frequency (continuous or intermittent), and intensity (mild or severe). As prey animals, horses may suppress pain to escape from imminent danger. This phenomenon, known as stress-induced analgesia, may have evolutionary significance and likely explains how a horse with a fractured limb continues to gallop after injury. In situations in which fleeing is not an option, violent or aggressive behaviors may be manifested. After the immediate danger is passed, however, heightened pain sensation such as allodynia (pain sensation caused by a normal stimulus) and hyperalgesia (heightened pain response to noxious stimuli) may help prevent further damage to already injured tissues. Allodynia and hyperalgesia can become pathologic and a disease unto themselves if they persist after resolution of injury. However, in an injured state, they are considered normal adaptive responses. Additionally, whether the animal is experiencing fear or anxiety may contribute to pain perception—recently, it has been reported that fear leads to analgesia, whereas anxiety leads to hyperalgesia. Because of the diverse nature of pain and unique species-specific considerations, assessment of pain is especially challenging in horses. To maximize accurate assessment, it is recommended that trained observers use a combination of subjective and objective measurements and use a consistent and systematic approach whenever possible. The horse’s normal temperament should be taken into account, for example, as should breed and age; older horses and draft horses may be more stoic, compared with Thoroughbreds and younger horses or foals. Those most familiar with a horse’s normal behavior, such as owners or grooms, should be consulted because they may be best qualified to identify abnormal behavior. When possible, the horse should be evaluated in its normal environment; strange environments may excite the horse, and isolation can cause stress, both of which can modify pain behavior. Evaluating pain is a staged process that begins with silent observation from afar. Clearly, a medical emergency is an exception that warrants immediate intervention. Observation from afar is important because horses may change or mask painful behaviors in the presence of humans. Use of video recordings may be very beneficial and, as in other domestic animals, can increase the accuracy of pain scoring. From afar, one should observe the horse’s general attitude, posture, limb placement, appetite, time spent exploring, and responsiveness to the environment. Evaluation of the horse’s immediate environment is important because it can indicate whether a horse is demonstrating normal or abnormal activity (e.g., the bedding is undisturbed versus notably displaced) and physiology (e.g., feces are formed in piles versus scattered around the stall or on the walls). After silent observation, the horse should be evaluated for response to and interaction with the observer. Finally, an interactive examination is performed in which physiologic parameters, including temperature, pulse and respiratory rate, noninvasive systemic arterial blood pressure (if possible), and frequency of borborygmus are recorded. Individually, these parameters may not provide a high level of sensitivity or specificity with regard to pain evaluation, but they may still be useful when considered along with other parameters. For example, tachycardia has numerous causes, but in a horse sedated with a large dose of an α2-receptor agonist (known to decrease heart rate), tachycardia is indicative of a significant problem, and pain should be high on the differential list. Additional parameters assessed during the interactive examination are dependent on the type and origin of pain and are discussed in more detail. To facilitate the practice of these principles, significant effort has been put forth to develop pain scales. A pain scale that incorporates the concept of a visual analog scale with objective findings, body posture, and facial expression has been developed at Colorado State University for use by faculty and staff. Although this scale has not been validated, it includes many of the aforementioned criteria (Figure 12-1). Another group developed a composite pain scale (CPS) to quantify orthopedic pain in an experimental model of tarsocrural synovitis using a combination of physiologic, interactive, and behavioral variables. This pain scale had good intraobserver and interobserver repeatability, sensitivity, and specificity. Of the parameters included in the CPS, posture, kicking at the abdomen, response to palpation, and interactive behavior all had good to excellent specificity; that is, these behaviors were not typically seen in horses not experiencing pain. Posture, head movement, kicking at the abdomen, pawing, response to palpation, and mean systemic blood pressure all had excellent sensitivity in differentiating among various pain levels. More recently, this CPS was used successfully in monitoring pain in horses with somatic or visceral pain caused by acute surgical and nonsurgical conditions. Nonspecific signs of pain may include restlessness, agitation, anxiety, a rigid stance, reluctance to move, lowered head position, fixed stare, dilated nostrils, clenched jaw, tail swishing, and aggression toward other horses, objects, or handlers. Horses in pain are less likely to interact with observers and explore the environment and are more likely to spend time at the back of the stall and avoid contact; they spend less time eating and less time in sternal recumbency, compared with horses not in pain. Horses in severe pain, regardless of the cause, are often restless, tachypneic, tachycardic, agitated, and profusely sweaty. Musculoskeletal pain can range from ill-defined mild stiffness to poor performance to complete non–weight-bearing lameness. If musculoskeletal pain is suspected, palpation to assess general muscle tone, digital pulses, and areas of heat, pain, or swelling is recommended. Response to palpation of a painful area is one of the most sensitive and specific pain parameters in horses. The muscles may be notably hypertonic, either as a guarding mechanism adjacent to the injured area or because of compensation for an abnormal gait. Limb pain may manifest as pointing of the affected forelimb, reluctance to move, stomping, alternate limb lifting and weight shifting, or an abnormal stance. For example, horses with navicular disease have been reported to point the more painful limb and may pack bedding under the palmar or plantar half of the foot to elevate the heels. Horses with acute foot pain, such as from an abscess, often have intense digital pulses and a warm hoof capsule; they may be sensitive to hoof testers or palpation of the coronary band in the region of the abscess. In horses that are ambulatory, a lameness examination should be performed. There are numerous subjective lameness scales available to aid in lameness evaluation, but in the United States, the scale published by the American Association of Equine Practitioners is the most commonly used (Table 12-1). This and other published lameness scales are subjective and lack a high degree of interobserver agreement. Efforts have been made to develop more objective means of measuring lameness, notably by the use of force plates to measure kinetics such as vertical ground reaction force, and with high-motion cameras that evaluate kinematics by use of reflective markers applied to the horse. Unfortunately, these systems are not readily available to most practitioners, and even in institutions that have the equipment and expertise, using them for clinical cases is often not practical. An exception to this is the Lameness Locator,1 a portable system that detects and quantifies asymmetries in body movement with the use of body-mounted inertial sensors and a gyroscope. This system is not yet in wide use, and although it is not designed to replace the equine lameness practitioner, it is a significant advance toward obtaining more objective lameness data. TABLE 12-1 American Association of Equine Practitioners Guidelines for Lameness Evaluation Copyright American Association of Equine Practitioners Guidelines for Lameness Evaluation, http://m.aaep.org/health_articles_view.php?id=280. Accessed February 7, 2014.
Recognition of Pain
Pain
General Guidelines for Assessing Pain
Nonspecific Signs of Pain
Assessing Specific Types of Pain
Musculoskeletal Pain
Grade 0
Lameness is not perceptible under any circumstances.
Grade 1
Lameness is difficult to observe and is not consistently apparent, regardless of circumstances (e.g., under saddle, circling, inclines, hard surface).
Grade 2
Lameness is difficult to observe at a walk or when trotting in a straight line but is consistently apparent under certain circumstances (e.g., weight carrying, circling, inclines, hard surface).
Grade 3
Lameness is consistently observable at a trot under all circumstances.
Grade 4
Lameness is obvious at a walk.
Grade 5
Lameness produces minimal weight bearing in motion and/or at rest or a complete inability to move.
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


