chapter 5 Radiographic Quality
Backscatter: Process of scattering or reflecting radiation in the opposite direction from that intended. Radiation that is reflected from behind the image plane back to the image.
Contrast: The measurable difference between two adjacent densities.
Crossed grid: Two parallel or two focused grids that are set at right angles. Also called crisscross grid.
Elongation: Distortion of anatomic structures so that the image appears longer than actual size, owing to the x-ray beam not being directed perpendicular to the film surface.
Focused grid: A grid with a parallel center lead strip and inclined strips on either side that radiate at progressively greater angles.
Foreshortening: Distortion of anatomic structures when the image appears shorter than actual size due to the plane of interest not being parallel to the film surface.
Geometric distortion: Variation in normal size and shape of anatomic structures due to their position in relation to the x-ray source and film.
Geometric unsharpness: Loss of detail due to geometric distortion.
Grid: A device made of lead strips embedded in a spacing material, placed between the patient and the film, designed to absorb non–image-forming radiation.
Grid cutoff: A progressive decrease in transmitted x-ray intensity caused by absorption of primary x-rays by the grid lines.
Grid efficiency: The ability of a grid to absorb non–image-forming radiation in the production of a quality radiograph.
Grid factor: The amount the exposure needs to be increased to compensate for the grid’s absorption of a portion of the primary beam.
Grid focus: The distance between the source of x-rays and the grid in which the grid is effective without grid cutoff.
Grid ratio: The relation of the height of the lead strips to the distance between them.
Linear grid: Grid in which the lead strips are parallel.
Lines per centimeter: The number of lead strips per centimeter area of a grid.
Magnification: Distortion of anatomic structures when the image appears larger than actual size.
Potter-Bucky diaphragm: A mechanical device that consists of a focused grid within a diaphragm, which moves the grid across the x-ray beam during the exposure.
Pseudofocused grid: A grid with parallel lead strips that are progressively reduced in height toward the edges of the grid.
Radiographic contrast: The density difference between two adjacent areas on a radiograph.
Radiographic density: The degree of blackness or “darkness” on a radiograph.
Radiographic detail: The definition of the edge of an anatomic structure on a radiograph.
Radiographic quality: The ease with which details can be perceived on a radiograph.
Scatter radiation: Non–image-forming radiation that is scattered in all directions because of objects in the path of the x-ray beam.
Subject contrast: The difference in density and mass of two adjacent anatomic structures.
Unfocused grid: A grid with lead strips that are parallel and at right angles to the film. Also called parallel grid.
INTRODUCTION
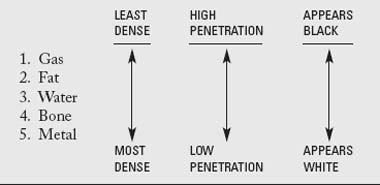
Radiographic quality refers to how easily details can be perceived on a radiograph. We must obtain as much diagnostic information as possible about the internal structures of the patient. Radiographic quality depends on radiographic density, contrast, and geometric factors that affect detail. This chapter will define diagnostic image characteristics and explain how to obtain them (Fig. 5-1).

RADIOGRAPHIC DENSITY
Factors Affecting Radiographic Density
Greater radiographic density may be produced by increasing (1) the total number of x-rays that reach the film, (2) the penetrating power of the x-rays, (3) the developing time, or (4) the temperature of the developer. (Film development is discussed in Chapter 7.)
As described in Chapter 3, the number of x-rays leaving the x-ray tube is determined by the milliamperage-seconds (mAs). As the mAs is increased, more x-rays reach the patient and film and radiographic density is increased. In the same respect, raising the kilovoltage (or kVp) of the x-ray beam increases radiographic density. As the kVp is increased, the penetrating power of the x-rays is increased, resulting in more x-rays reaching the film. The radiograph becomes darker as more x-rays reach the film.
Radiographic density is also influenced by the thickness and type of tissue being radiographed. Body parts that have greater thickness absorb more x-rays, resulting in a lighter image on the radiograph. Radiographic density is inversely proportional to tissue density. In other words, if the density or thickness of tissue doubles, the number of x-rays reaching the film is approximately halved. For example, the body of a 150-lb Saint Bernard will absorb many more x-rays than the body of a 75-lb Labrador retriever. Assuming that the same amount of x-rays was used for the Saint Bernard as required for the Labrador, the area of the film where the body of the Saint Bernard was located would be too white and would lack sufficient radiographic density to be diagnostic. In comparison, the radiograph of the Labrador would have adequate density because the correct exposure levels were selected for its body thickness (Fig. 5-2).

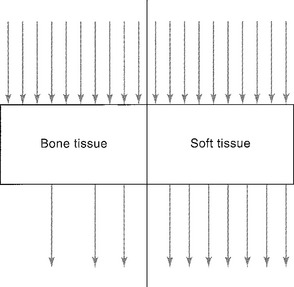
The body of an animal has many different types of tissues as well. Compare an animal’s bone with the surrounding muscle. Because the bone has higher tissue density than the muscle, more x-rays will be absorbed by the bone. The area of film under an anatomic area with high tissue density will be lighter (have less radiographic density). In other words, the area of the film where the bone was located will remain relatively white compared with the surrounding muscle tissue. Because x-rays have varied penetrability, the total number of x-rays reaching the film is partially dependent on the tissue density. Simply stated, the higher the tissue density, the lower the radiographic density (Fig. 5-3).
CONTRAST
Radiographic Contrast
Radiographic contrast is the density difference between two adjacent areas on a radiograph. When the density difference is great, the radiograph is said to have high contrast or a short scale of contrast. That is, a radiograph with high contrast exhibits many black and white tones. For example, a radiograph with white bone and a black background has high contrast (Fig. 5-4, A).
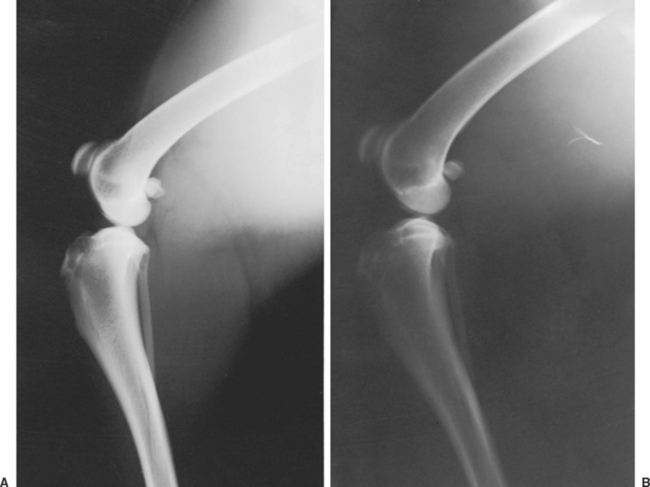
A radiograph that exhibits many grays and a small density difference between two adjacent areas has low contrast, or a long scale of contrast. An increased number of gray tones between the white and black tones on a radiograph constitute a long scale of contrast. In other words, it takes a long time to get from black to white on the radiograph. The type of contrast desired for each radiograph depends on the anatomic area (Fig. 5-4, B). General guidelines for desired contrast are listed in Table 5-1.
TABLE 5-1 GENERAL GUIDELINES FOR DESIRED CONTRAST
| TISSUE | CONTRAST | EXPOSURE FACTOR (KVP) |
|---|---|---|
| Bone | High | Low |
| Soft tissue | Low | High |
Of course, there are extremes in contrast. It is not desirable to have a radiograph with too high or too low of contrast (Fig. 5-5). A good radiograph should have a suitable range of differentiated radiographic densities (blacks, whites, and grays) so that the eye can easily see the detail.

Subject Contrast
As discussed earlier, the body has various tissue densities. Because x-rays cannot penetrate bone tissue as easily as soft tissue, fewer x-rays will reach the film where the bone is located. Bone will absorb many more x-rays than muscle or fat, assuming both have equal thickness. With appropriate exposure factors, anatomy that has high tissue density can increase the amount of whites and blacks on the radiograph; therefore high subject contrast increases radiographic contrast (Table 5-2).