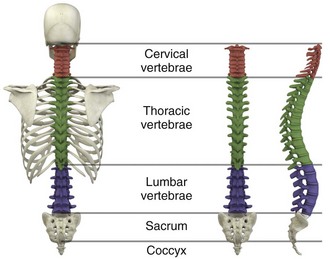
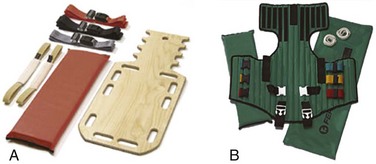
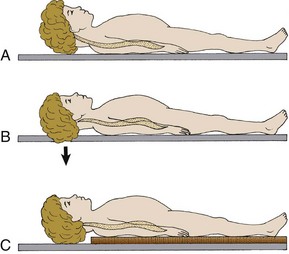
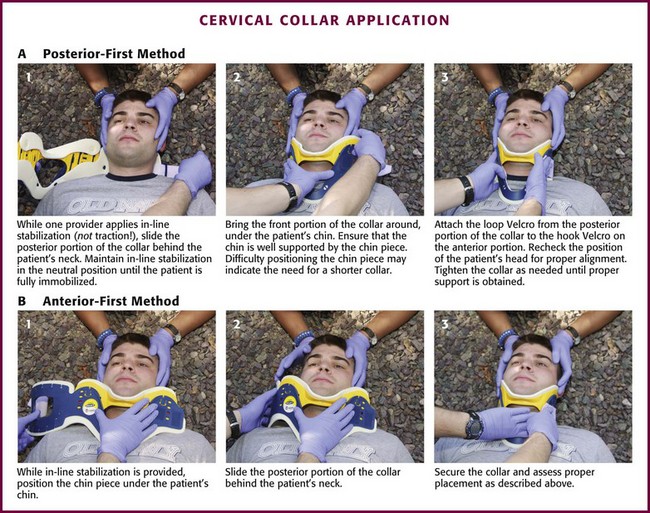
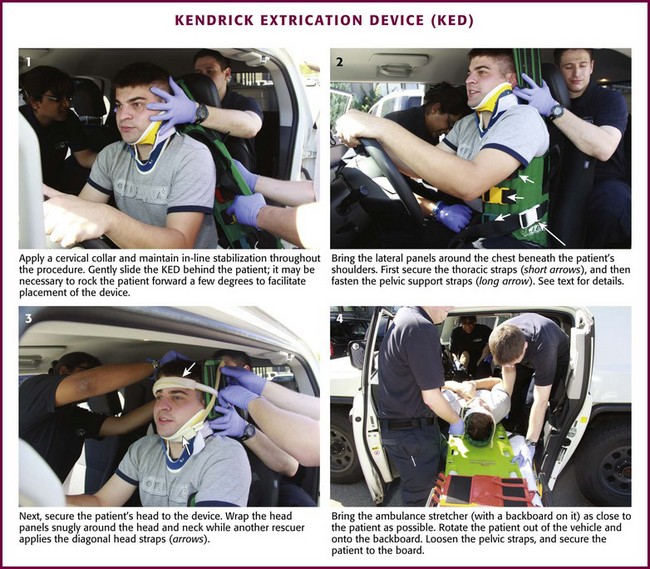
Chapter 46 The first recommendations for spinal immobilization following blunt trauma came from the American Academy of Orthopaedic Surgeons in 1971.1 These guidelines called for spinal immobilization of patients with symptoms or physical findings suggestive of spinal injuries.1,2 Since then, recommendations for spinal immobilization have evolved considerably. During the 1980s and 1990s, indications for spinal immobilization were based primarily on the mechanism of injury, regardless of the presence or absence of symptoms or physical findings suggestive of a spine injury.2,3 This resulted in routine prehospital spinal immobilization for all but the most trivial injuries and an abundance of unnecessary radiographs. Such wide-scale prehospital immobilization was initiated despite scant scientific evidence of improved patient outcomes. As a result, efforts were initiated to determine whether historical or clinical data could reasonably identify who had and who did not have serious injuries that would theoretically benefit from prehospital immobilization. Growing concern over the cost of cervical spine radiographs and excessive radiation exposure led to the development of easily applied low-risk criteria that could identify the vast majority of significant injuries in an attempt to safely reduce the overuse of cervical spine radiography.4 In early 2000, two large prospective studies validated the use of clinical criteria to rule out injury to the cervical spine in victims of blunt trauma.5,6 These studies dramatically reduced the number of unnecessary cervical spine radiographs following blunt trauma and led some investigators to question the prehospital practice of spinal immobilization based solely on mechanism of injury.2,7–9 In 1998, Hauswald and colleagues7 published the results of a 5-year retrospective review comparing patients from Malaysia, where cervical spine immobilization was nonexistent, to patients from New Mexico, where cervical spine immobilization based on the mechanism of injury was standard practice. Based on their results, the authors concluded that out-of-hospital immobilization has little or no effect on neurologic outcome in patients with blunt spinal injuries.7 More recently, researchers sought to determine whether prehospital providers could apply a set of clinical decision rules (Box 46-1) to selectively immobilize patients after blunt trauma.10,11 A 4-year prospective study in two Michigan counties found that the use of a selective immobilization protocol resulted in spine immobilization for most patients with spinal injury without causing harm to patients in which spine immobilization was withheld.10 A larger study in New York demonstrated that selective immobilization based on a statewide protocol resulted in only one nonimmobilized unstable cervical spine fracture in more than 32,000 patient encounters.11 Several other trials supported the use of clinical criteria for cervical spine clearance by prehospital care providers and hence supported the safety of avoiding routine immobilization for injuries that are extremely unlikely to be clinically significant.12,13 Although spinal fracture and spinal cord injury (SCI) can have devastating results, the incidence of such injuries in trauma patients is relatively low, about 2% to 5% in most reviews. Unfortunately, most final neurologic outcomes after spinal cord trauma can be prognosticated by the initial evaluation, and lifelong disability has been set by the primary insult, not by prehospital or emergency department (ED) interventions. Sundheim and Cruz14 calculated that only 0.03% to 0.16% of all out-of-hospital trauma patients may be expected to have secondary SCI that may be helped by immobilization. The number needed to immobilize to prevent one secondary injury is between 625 and 3333 trauma patients, but wholesale dismissal of any benefit from immobilization is not justified. It is important to note, however, that despite zealous use of prehospital cervical spine immobilization and countless medical and legal attempts to prove worsening of injury from its absence, there is little scientific evidence quantifying the effect of spinal immobilization in trauma patients or the possible adverse effects of its application (Box 46-2). Simply stated, the effect of spinal immobilization on mortality, neurologic injury, spinal stability, and adverse effects in trauma patients remains uncertain by evidence-based medicine, and no randomized prospective trials have been conducted. According to the National Spinal Cord Injury Statistical Center (NSCISC), an estimated 12,000 new, survivable SCIs occur in the Unites States annually.15 The NSCISC estimates that 265,000 people were living with SCI in the United States in 2010.15 Since 2005, the most common cause of SCI is motor vehicle collision, which accounts for just more than 40% of cases, followed by falls and acts of violence, primarily gunshot wounds.15 Sports such as American football, rugby, swimming and diving, gymnastics, ice hockey, track and field (specifically pole vaulting), cheerleading, and baseball all place participants at increased risk for spinal injuries.15 The cost of care in both the immediate and extended care setting can be exorbitant, especially among the young. The average lifetime cost of medical care for patients with SCI varies depending on the level of injury but ranges from 500,000 to more than 3 million dollars.15 The direction and strength of the injurious force may help predict the type of injury sustained. Generally speaking, the basic forces that can be exerted on the spine are flexion, extension, rotation, lateral bending, distraction (stretching), and compression (axial loading).16,17 Of course, complex mechanisms may exert multiple forces. For example, high-speed rollover motor vehicle collisions could easily exert all the aforementioned forces. Injuries to the upper cervical spine (C1 and C2) (Fig. 46-1) occur more often in older, osteoporotic patients than in younger patients. The spectrum of injuries in the cervicocranium includes occipital condyle fractures, occipitoatlantal dislocations, dislocations and subluxations of the atlantoaxial joint, fractures of the ring of the atlas, odontoid fractures, fractures of the arch of the axis, and fractures of the lateral mass of the axis (Fig. 46-2). Involvement of the spinal cord at this high level can cause devastating neurologic injury, and it is reasonable to believe that many of these injuries are not reported because they result in death.18 Subaxial cervical spinal injuries involving C3-7 have a broad spectrum of clinical implications. Approximately two thirds of cervical injuries causing quadriplegia occur within the lower cervical spine, with fractures occurring most often in C6 and C7 and dislocations most commonly occurring between C5-6 and C6-7.19 The orientation of the facets in the thoracic spine allows significantly less flexion and extension than in the cervical or lumbar spine. In addition, the free space between the thoracic spinal cord and the borders of the spinal canal is relatively small, and the blood supply is less robust. These factors increase the susceptibility of the spinal cord to injuries at this level. At the thoracolumbar junction there is an acute transition in stability because of the loss of rib restraint, which increases the risk for flexion-extension and rotational injuries. Disk size and shape also change, thus making this section of the spine particularly susceptible to injury. Approximately half of all vertebral body fractures and 40% of all SCIs occur between T11 and L2.20 The lumbar spine is protected only by the abdominal and paraspinous musculature, which makes it subject to distraction and shear forces, such as seen with lap belt injuries. There is also a higher prevalence of compression and burst fractures in the lumbar spine. These fractures commonly occur when axial loading forces straighten the natural lordosis at the moment of impact.21 The sacrum forms both the terminal portion of the spine and the central portion of the pelvis, which gives it added stability and makes isolated sacral fractures uncommon. Such fractures are usually caused by direct trauma or falls from a height or occur as a result of sacral insufficiency secondary to osteopenia, chronic steroid use, or previous pelvic irradiation. More often, sacral fractures occur as a result of high-energy mechanisms and are associated with major pelvic disruption.22 The National Association of EMS Physicians recommends spinal immobilization of prehospital trauma patients who sustain an injury with a mechanism that has the potential for causing spinal injury and who have at least one of the following clinical criteria: altered mental status, intoxication, a distracting painful injury (e.g., long-bone fracture), a neurologic deficit, and spinal pain or tenderness.2 Extremes of age and the presence of communication barriers (e.g., language, hearing impairment) may affect the ability to accurately assess the patient’s perception and communication of pain and should lower one’s threshold for spinal immobilization.2,3 It is also important to remember that serious cervical cord injuries can occur in the absence of demonstrable fractures. SCI is common in elderly patients with cervical spondylosis, in whom an arthritic osteophyte may sever a portion of the cord as permanently as a fracture or dislocation. In such cases there may be little subjective pain, and the mechanism of injury may appear seemingly minor.23 Spinal immobilization is contraindicated (or may require modification) when its use could harm the patient, when it is logistically impossible, or when the scene is unsafe (Box 46-3). Good clinical judgment, not blind application of protocols, is essential. For example, if application of a cervical collar will cause or mask airway compromise secondary to swelling, an expanding hematoma, or other process, it should not be used. Obviously, if a patient requires a surgical airway, the EMS provider will need immediate, unencumbered access to the anterior aspect of the neck. Sometimes preexisting airways (e.g., tracheotomy tube) and associated equipment prohibit proper application of a cervical collar. These situations can often be managed with an improvised cervical immobilizer, such as a collar fashioned from a towel roll or prolonged manual stabilization without traction. Other conditions that may prevent spinal immobilization or require modification of standard techniques and equipment (e.g., towel roll and manual in-line stabilization) include obesity, impaled objects, underlying respiratory problems or acute respiratory distress (e.g., from congestive heart failure or ascites), altered mental status (e.g., combative patients because of intoxication or psychiatric illness), and cervical dislocation with fixed angulation or anatomic limitations from preexisting conditions such as ankylosing spondylitis and kyphosis.24 There are also scenarios when spinal immobilization is logistically difficult or impossible. In a mass casualty incident, for instance, spinal immobilization of multiple victims with a low probability of spinal injury is impractical (Fig. 46-3). Finally, spinal immobilization may need to be delayed or modified when the scene poses a significant threat to the patient or providers (see Box 46-3).16 In these situations, the prehospital provider may opt for rapid extrication of the patient from the scene without immobilization of the spine (Fig. 46-4). Traditionally, cervical collars have used a four-point support structure at the bottom of the collar—at the two trapezius muscles posteriorly and at the two clavicles anteriorly. Most modern collars are modified rigid head-cervical-thoracic devices that use the sternum as a fifth support structure. Current collar designs support the head with winglike flaps on the collar’s upper posterior edges. Anteriorly, the collar supports the mandible. The collar’s flaring design generally prevents compression of the thyroid cartilage and cervical vessels, even when applied firmly. Some collars come as single units that conform to the neck once a chin support has been assembled, whereas others come in two parts, with a front and a back that are secured with Velcro (Fig. 46-5). Some manufacturers have developed collars that have adjustable heights to account for different neck lengths. Soft collars, though comfortable, have no role in spinal immobilization because they provide minimal support and do not reduce cervical motion to any significant degree.25,26 Investigators have attempted to evaluate cervical collars in an objective fashion. The accepted “gold standard” for comparison is the halo brace, which restricts motion to 4% flexion-extension, 1% rotation, and 4% lateral bending.27 Unfortunately, even the best cervical collars (when used independently) restrict flexion and extension by only 70% to 75% and overall neck movement by 50% or less.28 A number of studies have evaluated neck motion in volunteers immobilized supine on a backboard with various collars in place.25,26,29–32 Although these studies demonstrated small differences among some of the collars, overall they merely confirm the fact that cervical collars alone are inadequate to immobilize the cervical spine completely. Thus, it is important to keep in mind that for effective cervical spine immobilization, differences among the various types of cervical collars are less important than proper application, a snug but comfortable fit, and most importantly, use of adjunctive equipment. A large variety of short spine boards (Fig. 46-6) and intermediate-stage extrication devices are available for prehospital use. Generally, these devices are manufactured from rigid lightweight material. They have a narrow board design that permits easy application in automobiles or confined spaces and are constructed with multiple openings along the edges to allow a variety of strapping options. Ideally, these devices should also be translucent so that radiographs can be readily obtained in the ED, and they should allow repeated use and easy clean up. When not in use, store extrication splints with their straps secured in their individual retainers to reduce the likelihood of becoming entangled during application. One commonly used device that meets all these criteria is the Kendrick Extrication Device (KED) (see Fig. 46-6B). This device consists of two layers of nylon mesh impregnated with plastic and sewn over plywood slats to provide rigidity. It has a nylon loop behind the patient’s head that is continuous with the pelvic support straps for additional strength. Part of its anterior thoracic panels can be folded backward to fit obese, pregnant, or pediatric patients.33 When properly applied, the KED is a snug-fitting, highly adaptable immobilizer that can be used in even the most adverse circumstances. When patients require immobilization or extrication (or both) in more difficult or treacherous environments, many EMS providers prefer the LSP half-back, which resembles a KED but is more rugged and durable. In addition to providing spinal immobilization, it also acts as a harness and can be used for hauling patients over flat surfaces, as well as vertical lifts (Fig. 46-7).34 Mosesso and coworkers35 compared six prehospital cervical immobilization devices and concluded that the devices were similar in their ability to immobilize the cervical spine. Full-Body Spine Boards (Backboards): Backboards are made of wood or plastic composites and can be either rectangular or tapered in shape (Fig. 46-8A). Most rescuers prefer the tapered type because it takes up less horizontal room when angled into a narrow opening or doorway. In addition, the slight narrowing of these boards on either end enhances the effectiveness of strapping. The biggest drawback of using backboards as immobilizers is lack of patient comfort. Board splints, as a class, are the least comfortable of all immobilizers. Studies have demonstrated that spinal immobilization on a hard backboard causes head, back, and jaw pain.36,37 Pain in these areas may become severe if patients are left immobilized on these boards for extended periods.38–40 In addition, the pain caused by application of a backboard may be difficult to separate from other sources of pain in a trauma patient and might lead to unnecessary and costly radiographs.2 Discomfort may be minimized by using padding at points of contact between a bony prominence and the board. This concept was reaffirmed by Hauswald and colleagues,41 who found that increasing the amount of padding on a backboard decreases the amount of ischemic pain caused by immobilization. Scoop Stretchers: If an injured person has to be extricated from a tight location, a smooth backboard is probably the best device to immobilize and move the victim. If the victim is not in a tight location, the scoop stretcher is an ideal field immobilizer (see Fig. 46-8B). In fact, one recent study found that using the Sterno scoop stretcher caused less spinal motion than did a traditional long backboard and logroll technique.42 The scoop interferes slightly with the ischial section of a half-ring traction splint but works well with Sager-type devices. The Ferno-Washington model 65 scoop (Ferno-Washington, Inc., Wilmington, OH) is the most widely used stretcher of this type. Other devices such as the Combi-Carrier (Hartwell Medical, Carlsbad, CA) and the Scoop EXL (Ferno-Washington, Inc., Wilmington, OH) offer lightweight polymer construction and additional spine support (see Fig. 46-8C and D). Full-Body Splints: Various devices take the concept of full-body immobilization one step further than the spine board. One popular device is the Miller body splint, which consists of a polyethylene shell injected with closed-cell foam that is radiographically translucent and provides buoyancy in water (see Fig. 46-8E). This full-body splint features a removable head harness and a thoracic harness, as well as pelvic and lower extremity belts. The space between the lower extremities facilitates wrapping with bandage material in the event of fractures. In addition, it is shaped so that it can easily fit into a basket-type rescue stretcher. Similar spine immobilization systems are available for pediatric patients (e.g., Pedi-Pac, Ferno-Washington, Inc., Wilmington, OH). An important innovation in the area of spine immobilization in the United States has been the vacuum mattress splint (e.g., EVAC-U-SPLINT, Hartwell Medical, Carlsbad, CA, and Immobile-Vac, MDI, Gurnee, IL) (see Fig. 46-8F). It consists of a vinyl-coated polyester envelope filled with thousands of 1.1-mm-diameter polyester foam spheres. A manual or electric vacuum pump is used to evacuate the interior to a pressure of about 0.25 atm. This reduction in internal pressure causes the mattress to conform to the contours of the patient’s body. Vacuum splints have been shown to produce lower sacral interface pressure and lower mean pain scores than traditional hard backboards37,43 and may provide better immobilization in patients with known SCI.44,45 It should also be pointed out, however, that vacuum splints are larger and more cumbersome than backboards, thus making ambulance storage more difficult. Lateral Neck Stabilizers: Lightweight objects such as blocks (10 × 10 × 15 cm) made of medium-density foam rubber are commonly used to provide additional lateral stabilization of the head and neck. Foam blocks are inexpensive and disposable and do not slip on the backboard. Disposable cardboard devices that have the same advantages as foam blocks are also available (Fig. 46-9A). Another commercial device is the Universal Head Immobilizer. It is a lateral neck stabilizer designed to quickly and easily fasten the patient’s head to a scoop stretcher or spine board (see Fig. 46-9B). The Universal Head Immobilizer is made of a Herculite nylon and polyethylene foam platform fastened to the stretcher with Velcro straps. The lateral pillows are then attached to the nylon platform by means of large Velcro interfaces. Foam Padding: Padding increases comfort and can help prevent further injury. It can also help support an injured extremity or impaled object or allow an obese or kyphotic patient to lie supine on a long backboard (Fig. 46-10).29 Pregnant women may benefit from padding under the right hip to help shift the gravid uterus off the inferior vena cava and increase venous return.46 Padding applied under the neck and shoulders prevents hyperflexion in children with large occiputs (Fig. 46-11) or in individuals wearing certain types of helmets (e.g., bicycle, motorcycle, rock climbing) that cannot be removed in the field. The first priority in cervical spine immobilization is providing manual in-line stabilization in the neutral position. This can be done with the patient standing, seated, supine, or prone and consists simply of placing both hands on the sides of the patient’s head to prevent flexion, rotation, or bending. Do not apply cervical traction because it can increase the risk for SCI, and be sure to maintain manual in-line stabilization during application of the cervical collar and until the patient can be fully immobilized in an intermediate-stage corset-type device or on a long backboard (see later in this section). Once the cervical spine has been manually stabilized in the neutral position, examine the neck for swelling, ecchymosis, deformity, bony tenderness, or penetrating wounds. Application of a cervical collar follows and is generally a straightforward procedure (Fig. 46-12). The rescuer’s intentions should be thoroughly explained to the patient throughout the procedure. Once the collar is in place, conscious patients should be cautioned repeatedly against movement of the head. Investigate any persistent complaints of pain or dyspnea by removal and possible replacement of the device while manual stabilization is maintained. The size of collar should be determined from the manufacturer’s suggested guidelines. For example, the Stifneck collar (Laerdal Medical Corp., Wappingers Falls, NY) is available in various sizes and uses the distance from the top of the shoulder to the chin to determine the appropriate size. Use the tallest collar that does not cause hyperextension. For extremely short necks, a special cervical collar such as the No-Neck (Laerdal Medical Corp., Wappingers Falls, NY) is recommended. In cases in which a cervical collar of the proper size is not available, an improvised device should be made from available material (Fig. 46-13). It should also be remembered that application of a cervical collar should not be attempted until the patient’s head has been brought into a neutral position and manual in-line stabilization has been applied.28 If the patient experiences cervical muscle spasm, increased pain, neurologic complaints (e.g., paresthesias, weakness), or airway compromise, immediately halt any further movement of the head and neck. In these situations, immobilize in the position that the patient was found by using an alternative technique (e.g., blanket, towel roll, manual in-line stabilization). Sitting Position: To immobilize patients who are in a sitting position, use a short backboard or commercially available cervical extrication device (e.g., KED). At least two rescuers should be present to apply an extrication splint to a sitting patient. Interestingly, a recent study by Shafer and Naunheim found that healthy volunteers who were allowed to extricate themselves from the front seat of a car and lie down on a long spine board while wearing a cervical collar had less spinal movement than did those who were placed in cervical collars and moved onto the board directly or after application of a KED.47 Nevertheless, use of KEDs or short boards remains the most common method for vehicle extrication. Open the device butterfly style and gently slide it behind the victim via a rocking motion (Fig. 46-14, step 1). If necessary, carefully rock the patient forward a few degrees to facilitate placement of the splint. Once behind the victim, free the splint’s pelvic support straps from their retainers and allow them to dangle at the patient’s sides. Next, bring the lateral thoracic panels around the chest just beneath the patient’s shoulders. Grasp these panels and slide the splint upward until the top edges of the panels firmly engage the patient’s axillae. Now use the thoracic straps to secure the splint, beginning with the middle strap, then the bottom strap, and finally the top strap (see Fig. 46-14, step 2). Figure 46-14 Kendrick Extrication Device. Use of other short boards follows the same principles as depicted here. Next, secure the head to the device (see Fig. 46-14, step 3). When using the KED, wrap the head panels snugly around the head and neck while another rescuer applies the diagonal head straps. It may be necessary to place padding behind the head to maintain a neutral position. Use the forehead as a point of engagement for one strap and the cervical collar for the other. As a final step, tighten all buckles until the entire splint is firmly in place. The patient can now be moved. If the patient is to be lifted from a vehicle, bring the ambulance cot with a spine board on it as close to the patient as possible (see Fig. 46-14, step 4). While one rescuer supports the patient’s knees, the other rescuer uses the handholds on the splint to lift the patient. The patient should be rotated and laid in a supine position onto a backboard. Loosen the pelvic straps to allow the legs to be lowered onto the backboard. The legs can then be extended and secured to the backboard or left in the flexed position with a pillow placed under the knees for support. Recumbent Position: A patient who is found in a recumbent position should be placed in a supine position, if not already in one. If repositioning is necessary, examine the back during the process. Physical examination, spinal immobilization, airway management, and transport are easier to accomplish with the patient in the supine position. Scoop Stretcher.: A patient who is in a supine position can be moved by means of a scoop stretcher. In a conscious patient, rescuers should explain that they are about to apply a scoop-type stretcher, which may be cold to the touch, beneath the patient’s body. Apply a cervical collar and maintain manual in-line cervical stabilization until the patient is completely secured to the stretcher. Full-Body Spine Boards (Backboards).: There are several ways of placing a patient onto a spine board. The precise technique used will depend on the space available and the position of the patient within that space. For lengthwise extrication, as from an automobile seat, the patient can be slid, either feet first or head first, onto the backboard. It is important that the patient be moved as a unit during this process. Place one end of the backboard on the seat or doorsill of the automobile. One rescuer stabilizes the opposite end of the board while at least two other rescuers lift and slide the patient’s body onto the board. Once the patient is secured to the board, slide the board out of the vehicle and onto a waiting stretcher. Maintain manual cervical in-line stabilization throughout the procedure and avoid spinal compression or traction. When space permits, lateral extraction is preferred. If the patient is in the recumbent position, logroll or slide the patient onto the board. The logroll maneuver requires the presence of at least three rescuers. Position one rescuer at the patient’s head to apply manual in-line cervical stabilization (Fig. 46-15, step 1). It is this person’s responsibility to oversee and direct body movement throughout the procedure. Next, position the backboard next to the patient’s body (see Fig. 46-15, step 2). To minimize thoracolumbar movement, extend the patient’s arms at the sides with the palms resting on the lateral aspect of the thighs.48 To keep the patient from reaching for a rescuer or object during transfer, some rescuers prefer to have patients cross their arms across the thorax. However, this maneuver has not been shown to prevent or minimize thoracolumbar movement. If one arm is injured, place the backboard against this side so that the patient can be rolled onto the uninjured extremity. Position the other rescuers on the side that the patient will be rolled toward, with one rescuer at the midchest level and the other at the legs. The rescuer at the chest should reach across the victim and take hold of the shoulder and hips while the other rescuer grasps the hips and lower part of the legs. When everyone is ready, the rescuer at the head gives the command to roll the patient onto the side (see Fig. 46-15, step 3). If possible, examine the patient’s back at this point. Slide the backboard under the patient, and when everyone is ready, the rescuer at the head gives the command to roll the patient back onto the board (see Fig. 46-15, step 4). Before applying straps, it is often necessary to center the patient on the board.
Prehospital Immobilization
Spine Immobilization
Epidemiology
Pathophysiology
Indications
Contraindications
Equipment
Cervical Extrication Splints
Full-Body Spine Immobilizers
Procedure
Thoracolumbar Spine Immobilization
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree