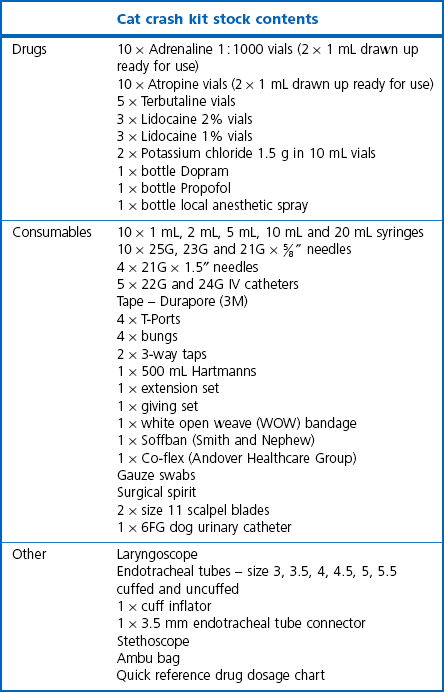
Chapter 4 Nursing care is defined by the American Association of Feline Medicine (AAFM) and the International Society of Feline Medicine (ISFM) as any interaction between the cat and the veterinary team (veterinarian, technician or nurse, receptionist or support staff) in the clinic, or between the cat and its owner at home, that promotes wellness or recovery from illness or injury and addresses the patient’s physical and emotional well-being.1 Nursing care also helps the sick or convalescing cat engage in activities that it would be unable to perform without help. To provide optimal support to a sick, injured or recovering cat, the art of nursing care is as important as the medical science.1 The postoperative care of a cat should not be neglected; attention to this aspect of the cat’s treatment can make a big difference to the nature of the recovery and well-being of the patient. In some cases the provision and quality of postoperative care can mean the difference between a successful and unsuccessful outcome. This chapter will focus on the provision of nursing care for the postoperative period up until and including discharge of the recovering cat to the owner (for other aspects of postoperative management and monitoring see Chapter 3). Short sections are included on the pertinent points on provision of nursing care of cats, which have undergone skin and adnexal surgery, abdominal surgery, thoracic surgery, and head surgery. The recovery period can be the most critical stage of anesthesia for a cat. Current estimates indicate that approximately 0.11% (1 in 895 anesthetics) of healthy cats die of an anesthetic-related death, which is more than twice as frequent as has been recently reported in dogs (0.05% or 1 in 1849). Most of these deaths occur in the postoperative period.2 Greater attention to patient monitoring during and after anesthesia could reduce perioperative complications in cats;2 the recovery area should be appropriately equipped and have trained personnel monitoring recovery of patients after anesthesia and surgery. Obstruction of the airway due to fluid or mucus is a common cause of acute hypoxia during the recovery phase.3 If obstruction is suspected the airway should be carefully aspirated. A suction device is an essential piece of equipment for the ICU. In cases where an airway cannot be established, due to an obstruction for example, an emergency tracheostomy may need to be performed (Chapter 46). Alternatively, a large gauge needle can be inserted directly into the trachea to allow immediate oxygenation until a tracheotomy can be performed. A fully stocked emergency box should be kept in the recovery area. This should be checked weekly and replenished after every use. It is important to ensure all members of staff know where the emergency box is kept and that it is kept within easy access. The contents of the box should be set out clearly and the box should not be overcrowded with drugs and equipment, so that anyone using it can locate what they need quickly and efficiently. To avoid overloading the general emergency box, it can be helpful to have smaller kits for specific procedures made up ready for use, for example for thoracocentesis (Chapter 41) or tracheotomy (Chapter 46). To minimize preparation time, commonly used emergency drugs e.g., adrenaline (epinephrine) and atropine, can be kept drawn up in syringes ready for immediate use. However, this is not appropriate for all emergency drugs, as not all drugs contain preservatives and so will lose effectiveness once the vial is opened. It is therefore important that expiry dates are checked and adhered to. Having some syringes with suitable sized needles already attached in the emergency box can save time when drawing up drugs. An easy-to-follow emergency ‘drugs and dosage’ chart is also invaluable to ensure there is minimal delay in administering the correct drug and dose in an emergency situation. Essential recommended items for a feline emergency box are listed (Table 4-1). Thorough and attentive patient assessment and monitoring with effective communication of the findings can facilitate excellent patient care and an optimal recovery (Fig. 4-1). After any surgery the cat should be assessed for certain signs, parameters, behavior and functions (Box 4-1), the relevance and importance of each being dependent on the surgery performed. Figure 4-1 Heat loss should be minimized during anesthesia. (A) The cat is on a heat pad in the operating theatre. (B) This cat is being kept warm in the radiology room by use of bubble wrap and a towel. A cat’s vital signs should be interpreted in conjunction with environmental factors and the temperament of the individual cat. The presence of pain can result in elevations in pulse and temperature. The significance of a high pulse count and respiratory rate should be evaluated along with the cat’s other parameters (temperature, pulse quality, mucous membrane color, capillary refill time, respiratory pattern etc.), as well as assessing if the cat is stressed or fearful (Chapter 7). Stress and fear will give falsely high pulse and respiration rates so it is important that the cat’s environment should be evaluated to determine, for example, whether the proximity of a dog or another cat is causing these elevations. Once the cat has recovered from anesthesia, the frequency of monitoring and which vital signs are important to monitor will depend on the surgery that has been performed, how well the cat recovered from the procedure, how it is progressing clinically and how tolerant the patient is (Chapter 7). A low body temperature may both increase the chance of postoperative infection through immune function suppression and delay recovery from anesthesia. Most postoperative cats will be hypothermic to a degree, and therefore it is of utmost importance to monitor the temperature during the recovery phase and quickly implement methods of restoring normothermia before further temperature reductions occur. To prevent or minimize postoperative hypothermia in the recovery room provision should be made first to keep cats warm while under anesthesia (Fig. 4-1). Cats in the recovery area can then be warmed by warm air blankets (Bair Huggers), a warming mat, bubble wrap, blankets, warm gloves, warm bean or rice bags. While being warmed the cat’s temperature should be monitored regularly to avoid hyperthermia. In addition to excessive warming, hyperthermia in cats in the postoperative phase is also seen with opioid administration, including hydromorphone, morphine, butorphanol and buprenorphine.4 The increase of temperature seen is usually mild to moderate (<40.1°C [104.2°F]) and self-limiting.4 If the cat is hyperthermic due to overheating, infection or opioid administration and this is of concern, the cat should be judiciously cooled by removing all warming aids in the first instance. If hyperthermia still does not resolve then other methods of cooling can be considered such as the use of fans, or the application of surgical spirit to the foot pads in combination with continued temperature monitoring. Reversal of the opioid can be achieved by administering naloxone, but this will also remove the analgesic effect of the drug, so alternative pain therapy will be required. The assessment of pain is an essential skill that should be acquired by all personnel involved with the postoperative recovery of cats. Recognition of pain in cats is challenging as the signs are often more subtle than in dogs.5 Cats show mainly postural signs, without vocalization.6 To make things even more difficult, many of the signs of pain that cats show are also displayed when they are fearful and so it can be very challenging to differentiate between the two (Box 4-2). An initial assessment should begin by observing the cat in its cage from a distance. Cats that are happy and pain free will be alert, responsive and move freely around the cage with no signs of distress. Cats that are in pain will be quiet and withdrawn and may well be hunched up at the back of their cage. They will not usually move around freely or respond when called or spoken to. The environment should also be taken into consideration; if the cat is in a ward with barking dogs or if the cat has a nervous disposition it may display similar signs to that of a cat in pain. After the initial assessment of observing the patient from a distance has been completed, the cage door can then be opened. The cat can be talked to and gently stroked. Pain-free cats tend to respond well to this interaction. Some cats will get up and approach the assessor and even nervous cats will sometimes raise their hind quarters when being tickled at the base of their tail. Very fearful cats may growl or show aggression and not allow any physical contact, but this behavior is not necessarily related to pain. The area peripheral to but in close vicinity to the surgical site, should then be gently palpated. In any assessment of pain mere observation is insufficient and interactive means such as palpation must also be used.7 Changes in wound sensitivity have correlated well with visual analog pain scores in cats, suggesting that palpation, which is a simple clinically applicable technique, is a valuable tool and should be incorporated into an overall assessment protocol.8 A painful cat will become tense, look uncomfortable and may flinch or vocalize during palpation. Some cats will also hypersalivate in response to pain. If these signs are shown palpation should be stopped immediately until more analgesia has been administered. Box 4-2 Behavioral and physical signs that may be exhibited in painful and fearful cats Tense and hunched posture – body low to the ground, limbs tightly kept towards the body, often pressed up against the back of the kennel or in their litter tray An unwillingness to interact with people Eyelids pointing down (like the cat is frowning) Ear position starting to turn then flatten Whiskers flattening then coming forward immediately before aggression Reduced urine and fecal output
Postoperative nursing care
Recovery from anesthesia
Emergency anesthesia equipment
Emergency box
Principles of postoperative nursing care


Basic parameters
Temperature
Pain recognition
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Postoperative nursing care