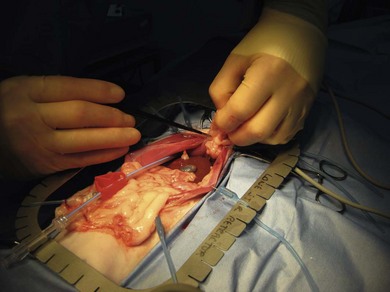
Chapter 23 Surgical exploration of the abdomen can provide invaluable information to help achieve a diagnosis of a large number of disease processes. Progress in the fields of imaging, minimally invasive biopsy techniques, and endoscopy and laparoscopy (Chapter 24) has significantly reduced the indications for open exploration of the abdomen. Despite these techniques, the ability of the surgeon to perform both a visual and manual examination of all abdominal organs and obtain biopsies from multiple sites during open exploratory surgery can be invaluable.1–3 Celiotomy refers to an incision into the abdomen; laparatomy, a term often used interchangeably with celiotomy, can also refer to surgery performed through a flank incision, which is rarely performed in cats except for ovariohysterectomy. Exploratory celiotomy cannot be considered a benign procedure and therefore, whenever possible, the clinician should ensure that all other diagnostic possibilities have been considered prior to surgery. While the limitations of preoperative diagnostic procedures should be appreciated (ultrasonography failed to identify the causative pathology in 25% of cases in one study4), preoperative investigations can reduce the incidence of unnecessary surgery and should minimize the risk of ‘peak-and-shriek’ intervention where the pathology proves to be beyond the experience level of the surgeon. At the very least, the principal surgeon involved in an exploratory procedure should be familiar with and have the necessary equipment available to assess and biopsy any abnormal tissue. In addition to facilitating a global assessment of the abdomen and biopsy of tissue, in some cases the exploratory celiotomy also offers the opportunity to treat the pathology.2,3 It is inevitable, therefore, that the experience and competence level of the surgeon in recognition of abnormality, application of biopsy techniques and in the surgical treatment of disease will have an impact on whether the procedure can be judged as a success. A more detailed account of the abdominal anatomy of the cat is provided in the chapters on the relevant organs (see Chapters 27 to 40). In this section, for the benefit of the surgeon who is more accustomed to operating on the dog, anatomical differences between the feline and canine abdominal cavity and viscera that are relevant to exploratory celiotomy surgery will be briefly highlighted. The liver consists of seven major lobes, which in the cat are separated by particularly deep fissures, rendering them more mobile relative to each other than in the dog.5 The feline gallbladder is situated between the right medial and quadrate lobes as in the dog and can be double as a normal variation.6 The cystic duct of the cat is usually longer and more undulating in its course than in the dog, and the common bile duct shares a common opening at the major duodenal papilla with the dominant pancreatic duct (see below).5 The pancreas is similar in appearance to its canine counterpart and occupies the same anatomical location and blood vessel arrangement as in the dog. Drainage of secretions from the feline exocrine pancreas differs in two respects from the situation in the dog, the first being that most cats (approximately 80%) only have one duct, with the result that all of, or the significant majority of, the secretions enter the duodenum at the proximal (major) duodenal papilla (the canine pancreas drains predominantly via the minor duodenal papilla). The second difference is that the pancreatic duct can join with the common bile duct in cats and therefore share the same opening into the duodenal lumen.5 These differences combine to make both the common bile duct and pancreatic duct prone to secondary obstruction in the presence of disease involving the region of the major duodenal papilla. The left renal artery can divide before it enters the kidney (resulting in two or more renal arteries) in approximately 10% of cats.7 The right renal artery usually remains undivided outside the capsule. The vessels running over the surface of the renal capsule (both arteries and veins) are significantly more prominent in the cat than in the dog. Venous drainage occurs into the caudal vena cava via the renal veins. There are commonly several renal veins visible at the feline hilus, particularly on the right-hand side.8 Retraction of the abdominal wall can be performed by mini Balfour, Gosset, Gelpi, or other self-retaining retractors (Chapter 13), ensuring that no viscera become trapped between the retractor and the body wall. Moist swabs or laparotomy swabs are used to protect the abdominal wall from trauma that can be caused during retraction. Lightweight self-retaining retractors with elasticated hooks are versatile and can be very useful in small animals due to their reduced weight (Fig. 23-1). Excision of the falciform fat can be very helpful in gaining unimpaired access to the cranial abdomen in some cats (Fig. 23-1) and can be performed with judicious use of electrocautery or bunch-ligation at its cranioproximal extent. Figure 23-1 A versatile lightweight retractor in position during excision of the falciform fat using bipolar diathermy forceps. There is a transdiaphragmatic thoracic drain in place. Abdominal exploration includes evaluation of the abdominal surface of the diaphragm, the distal extent of the esophagus, the entire stomach, duodenum, jejunum, ileum, colon, cecum, pancreas (both limbs), liver, gall bladder, kidneys (the duodenal and colonic maneuvers are useful; Figs 23-2 and 23-3), ureters (observe peristalsis if relevant), bladder and proximal urethra, and any genital organs that are present or likely to be relevant. Table 23-1 gives details of a suitable approach to abdominal exploration although other techniques have been described.9 Table 23-1 Example of a protocol to achieve systematic exploration of the abdomen Figure 23-2 The duodenal maneuver. The right kidney and associated vasculature are visible. Retention of the remainder of the abdominal viscera was achieved using the mesoduodenum as a ‘dam’. The duodenum is grasped gently, ensuring that the right limb of the pancreas is not damaged. The pancreatic appearance was not associated with clinical signs and was considered acceptable.
Celiotomy
Surgical anatomy
Liver
Pancreas
Urogenital system
How to perform an exploratory celiotomy
The exploratory celiotomy
Area of exploration
Technique
Gastric cardia, distal esophagus, left diaphragm, cranial pole of the left kidney and left adrenal gland
The left medial and lateral liver lobes are retracted towards midline to reveal the diaphragm and distal esophagus. Both surfaces of the left side of the liver can be assessed. The colonic maneuver (described below) can be used to increase exposure of the left kidney and adrenal gland if necessary
Right liver lobes, right diaphragm
The quadrate, right medial and right lateral liver lobes are retracted towards midline. The surgeon can then palpate and assess those liver lobes, and make a visual inspection of the surface of the right diaphragm
Gall bladder and extrahepatic biliary system. Portal vein
The stomach is then retracted caudally slightly, facilitating inspection of the gall bladder, cystic duct and common bile duct. Great care is taken over performing or interpreting manual gall bladder emptying due to the potential for reflux into the hepatic ducts
Gastric assessment
The entire stomach is then palpated, including the fundus, body, pyloris and assessment continued to include the proximal duodenum. The proximal duodenum is tethered by the duodenohepatic ligament
Pancreas
The right limb of the pancreas is elevated by grasping the descending duodenum. Care is required in order not to handle the pancreas excessively. The left pancreatic lobe can be inspected by reflecting the greater omentum ventrally and cranially or opening the omentum itself
Small intestines
The duodenum is followed to the duodenocolic ligament that tethers it to the dorsal abdomen. A loop of jejunum is grasped and followed in one direction. The surgeon will then either encounter the distal duodenum and duodenocolic ligament again or the ileocecocolic junction. The surgeon then proceeds by following the jejunum in the other direction from the start point. The ileum is identified by its antimesenteric vessel
Large intestines
The cecum can be palpated and inspected along with the ascending, transverse and descending colon. The proximal ascending colon is relatively immobile as it is secured dorsally in the abdomen by the duodenocolic ligament
Proximal urinary tract
Duodenal maneuver: the descending duodenum is grasped, taking care to avoid handling of the pancreas, and the mesoduodenum is used as a barrier to gently retract the jejunum etc. towards midline. The right kidney, adrenal gland and proximal ureter can be examined, palpated if appropriate and observed. A similar maneuver making use of the descending colon and mesocolon (colonic maneuver) will allow inspection of the left kidney
Distal urinary tract
The bladder is palpated and reflected ventrocaudally to inspect its dorsal surface and ureteric insertion points. The neck of the bladder can be gently palpated
Genital system
The ovaries or stumps should have been visualized during the duodenal or colonic maneuvers. The uterus or uterine stump(s) can be identified/palpated dorsal to the bladder and ventral to the colon, assisted by caudoventral retraction of the bladder if necessary

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Celiotomy
