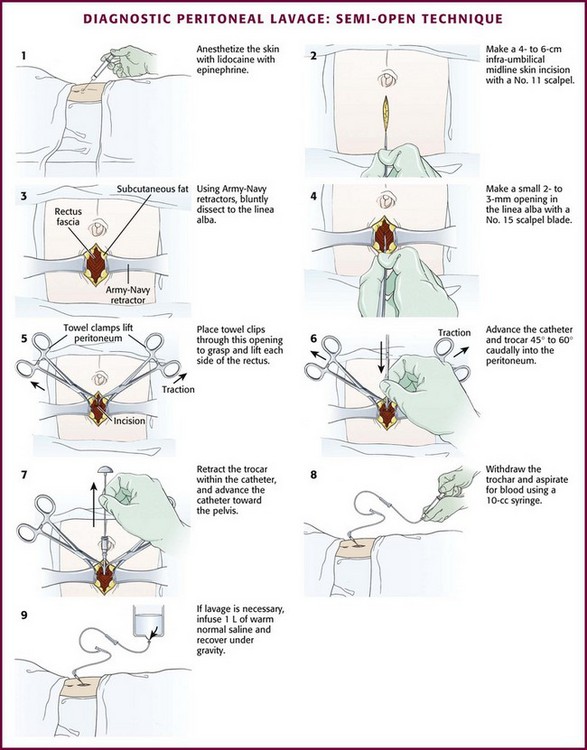
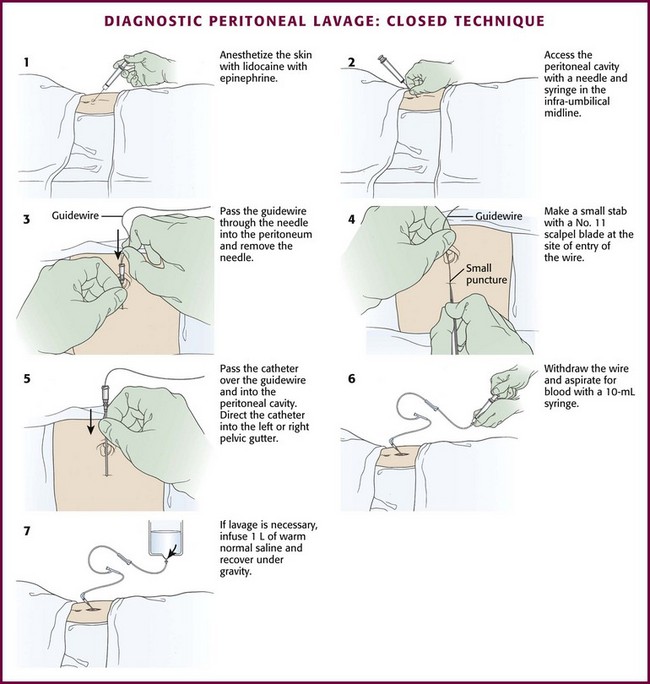
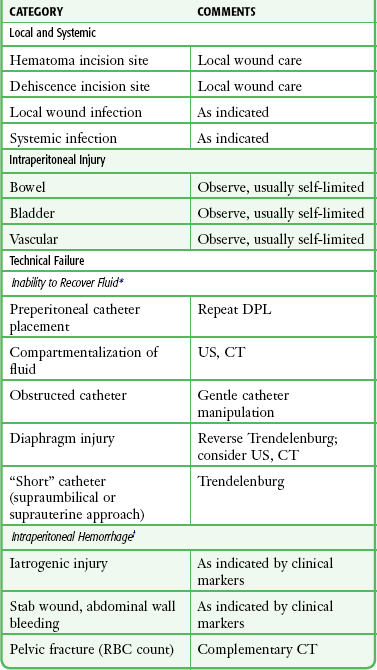
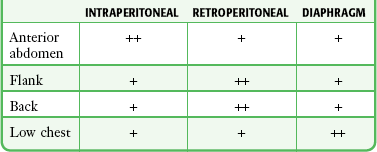
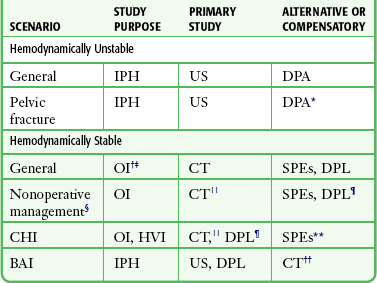
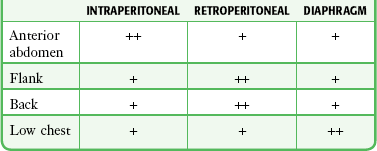
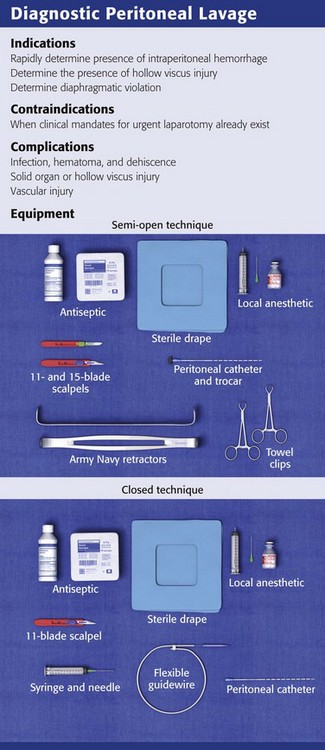
Chapter 43 Root and colleagues introduced DPL in 1964.1 It has withstood the passage of several decades and remains a useful diagnostic adjunct for the management of penetrating torso trauma. Following a blunt mechanism of injury, its greatest utility is as a triage tool in the assessment of hemodynamically unstable, multiply injured patients. The intent is to rapidly discover or exclude the presence of intraperitoneal hemorrhage (IPH). The advent and availability of ultrasound (US) in the emergency department (ED) have rendered this purpose complementary to that of US in the diagnostic armamentarium of emergency clinicians evaluating blunt trauma patients.2 Peritoneal lavage can be used as a therapeutic tool in patients with hypothermia and as a means of removing toxins.3 It has also been used as a diagnostic instrument for suspected intraabdominal infection and nontraumatic sources of hemorrhage.4,5 Although the steps of the procedure are the same regardless of the indication, the primary use of DPL is to determine the need for laparotomy after trauma, and this chapter focuses on that indication. Before the advent of computed tomography (CT) and US, DPL was the sole diagnostic option to supplement physical examination for predicting the need for operative intervention (Table 43-1). It was integral to both reduction of unnecessary laparotomies and discovery of unsuspected and life-threatening intraabdominal hemorrhage in patients with significant closed-head injury.6,7 TABLE 43-1 Clinical Indications for Laparotomy after Blunt Trauma From Marx J, Isenhour J. Abdominal trauma. In: Marx JA, Hockberger RS, Walls RM, et al, eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 6th ed. St. Louis: Mosby; 2006:509. This procedure may be undertaken by the emergency physician, but its use is not mandated and often relegated to the trauma service or consulting surgeon. In a number of respected centers in the United States, DPL continues to be a focal diagnostic instrument.2,8 It serves two primary functions.9 First, it can be used to rapidly determine or exclude the presence of IPH (Table 43-2). Thus, a patient with a critical closed-head injury, an unstable motor vehicle crash victim with multiple potential sources of blood loss, or a patient with pelvic fractures and retroperitoneal hemorrhage can be appropriately routed to lifesaving laparotomy.10,11 Furthermore, given its exquisite sensitivity, a negative peritoneal aspiration allows the clinician to proceed to alternative management steps and the patient to forego unnecessary laparotomy. Second, DPL has been used in less exigent circumstances as a means of predicting solid or hollow visceral injury requiring laparotomy.12,13 However, in this venue its sensitivity to the presence of hemorrhage may prompt unnecessary laparotomy in patients with self-limited lacerations of the liver, spleen,14–17 or mesentery.17 CT specifically evaluates all intraperitoneal structures, as well as the retroperitoneum, a region inaccessible to DPL. Because the resolution and the speed with which it can be undertaken have vastly improved, CT has become an invaluable adjunct in the management of blunt trauma and has largely replaced DPL in stable patients. It is most useful in identifying injury to solid organs with accompanying IPH and greatly assists nonoperative management of these injuries. The ability of CT to discern hollow viscus and pancreatic pathology has continued to improve as the modality has evolved.11 With regard to hollow viscus injury, it is when serial clinical evaluations cannot be performed that gut perforation leads to preventable mortality. This is especially true in patients with severe closed-head injury or high spinal cord injury, in whom physical assessment of the abdomen is quite compromised. It is for these express scenarios that some authorities recommend the performance of DPL. The clinician’s concern for hollow viscus injury should be heightened if US or CT demonstrates minimal amounts of free intraperitoneal fluid without evidence of solid organ damage.18 TABLE 43-2 Likelihood of Injury by Entry Site From Marx JA. Diagnostic peritoneal lavage. In: Ivatury RR, Cayten CG, eds. The Textbook of Penetrating Trauma. Baltimore: Williams & Wilkins; 1996:336. Two paradigms have brought US to the forefront. First, this modality has been adopted as the primary triage instrument, in lieu of DPL, for the detection of IPH on the basis of identifying which pouches and gutters are filled with fluid.19–21 Clinical success in this role has been mixed, with reported sensitivity for IPH of 65% to 95%.22–28 In addition, to be useful in this role, a competent technician and interpreter and the appropriate equipment must be present in real time. It has been demonstrated that emergency clinicians and surgeons can be trained in this technique to a level of competence sufficient for this need.29 In centers that rely on US, DPL should serve as a reliable study when US equipment is unavailable, performance of US is technically difficult, or the results of US are indeterminate, especially when the patient demonstrates hemodynamic compromise. DPL is a readily available procedure that can be conducted rapidly in the safe confines of the ED. The ability to undertake CT in particular or, to a lesser extent, US in a similar manner requires careful consideration of the clinical circumstances, location of equipment, and capabilities of the personnel available (Fig. 43-1 and Table 43-3).2,11 TABLE 43-3 Diagnostic Studies in Patients with Blunt Abdominal Trauma *A positive peritoneal aspirate mandates laparotomy; a positive red blood cell count warrants attention only to the pelvic fracture. †To discover fluid or blood suggesting injury. ‡US for OI is much less reliable than for IPH. §Institutional capability should be carefully considered. ||CT is less reliable for HVI than for solid visceral injury. ¶Complementary to CT if HVI is suspected. **SPEs are unreliable in patients with CHI. ††May be more appropriate if helical CT is the primary study for BAI or can be acquired rapidly. Adapted from Marx J, Isenhour J. Abdominal trauma. In: Marx JA, Hockberger RS, Walls RM, et al, eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 6th ed. St. Louis: Mosby; 2006:507. The advent of DPL was seminal in the promotion of selective management for penetrating abdominal injury. Here its role is more dominant than for blunt trauma because of the far greater likelihood of occult injury to hollow viscera and the diaphragm after a penetrating mechanism.30,31 Instruments and missiles may penetrate the abdominal cavity via the anterior abdominal wall, flank, back, or low chest region.32 The intraperitoneal space is vulnerable if penetration occurs as high as the fourth intercostal space anteriorly and the sixth or seventh space laterally and posteriorly because the diaphragm may rise to these levels in the expiratory phase of respiration.33 Coincident thoracic penetration occurs in up to 46% of patients with abdominal injuries.34–36 The likelihood of retroperitoneal injury increases when the entry site is over the flank or back, but the prospect of intraperitoneal pathology remains considerable, with cited incidences of up to 43% for the flank and 14% for the back (Table 43-4).37–39 TABLE 43-4 Likelihood of Injury by Entry Site From Marx JA. Diagnostic peritoneal lavage. In: Ivatury RR, Cayten CG, eds. The Textbook of Penetrating Trauma. Baltimore: Williams & Wilkins; 1996:336. Stab Wounds: Because only one fourth to one third of patients who sustain stab wounds to the anterior aspect of the abdomen require laparotomy, diagnostic algorithms are used to decrease the rate of unnecessary surgery.30,35,40 An optimal approach would not sacrifice sensitivity for morbid intraperitoneal injury. A pathway using a combination of clinical mandates, local wound exploration, and DPL is well established (Fig. 43-2).41 These clinical mandates are reasonably accurate predictors of significant intraperitoneal injury (Table 43-5). Thus, the presence of one or more mandates suggests the need for urgent laparotomy and precludes the undertaking of other diagnostic studies. TABLE 43-5 Clinical Indications for Laparotomy after Penetrating Trauma Modified from Marx JA. Diagnostic peritoneal lavage. In: Ivatury RR, Cayten CG, eds. The Textbook of Penetrating Trauma. Baltimore: Williams & Wilkins; 1996. DPL fills three roles in the evaluation of patients with abdominal stab wounds (see Table 43-2): (1) rapid determination of the presence of hemoperitoneum, (2) discovery of intraperitoneal injury requiring surgery in stable patients, and (3) establishment of diaphragmatic violation. As is the case in blunt trauma patients, DPL can be invaluable as a rapid triage tool when the source of hemodynamic instability is not known. Pericardial tamponade, intrathoracic hemorrhage, and IPH may be contributory to hemodynamic instability or wholly causal. Again, as for blunt trauma evaluation, US is the only bedside diagnostic modality for IPH that is competitive in this role, and it carries the added advantage of scanning for intrapericardial and intrathoracic hemorrhage.35 In determining injury after stab wounds, DPL has 90% accuracy.42–44 Serial examinations,45–47 CT, and laparoscopy48–51 are alternative modalities in specific circumstances and centers.52 The diaphragmatic rents created by stab wounds are generally small; thus, at the outset they do not create apparent clinical or radiologic abnormalities.53,54 However, morbidity from delayed herniation of bowel is common and substantive.55 Physical examination is notoriously insensitive and DPL is currently the most sensitive means of discerning this injury in the immediate posttrauma phase.42 There is some evidence that coronal reconstruction of CT images provides greater sensitivity for detecting small diaphragmatic tears, and as CT technology continues to evolve, it may surpass DPL for evaluation of these subtle injuries.56 For these small wounds, magnetic resonance imaging may be diagnostic, but because of safety and accessibility concerns, it should be reserved for the nonacute phase of management. Laparoscopy has demonstrated promise in experienced hands.48,49 Gunshot Wounds: Injury to multiple organs is the rule after gunshot wounds, and mortality is significantly greater than after stab wounds.52 The diagnostic approach is more conservative for gunshot wounds because in some studies the likelihood of intraperitoneal injury requiring operative intervention has exceeded 90% when the projectile has entered the intraperitoneal cavity (Fig. 43-3).57 If clinical mandates are met (see Table 43-5) or if peritoneal violation has occurred, most centers proceed to laparotomy.41 One series, however, cited intraabdominal injury in 70% to 80% of cases, thus supporting the contention that nonoperative management could be applied to a substantial percentage of patients.58 In a separate cohort of 152 patients sustaining solid organ injury from penetrating abdominal trauma (70% gunshot wounds and 30% stab wounds), 27% were successfully managed without laparotomy after selection by a protocol combining clinical examination and CT scanning.59 DPL is reserved for two circumstances: (1) the wound tract is neither obviously superficial nor intraperitoneal, and (2) penetration occurred in the low chest region, where diaphragmatic injury is more likely yet the possibility of intraperitoneal injury also exists. Decompress the stomach and bladder to prevent inadvertent injury. Place the patient in the supine position and administer sedatives and analgesics as appropriate. Perform DPL according to compliance with standards for body fluid precautions. Observe sterile technique throughout the procedure. Before making the skin incisions described later, prepare the site with standard skin antiseptics and drape appropriately. Prophylactic antibiotics are not indicated for routine DPL because local and systemic infections are rare.60 Infiltrate the area for incision and dissection with a local anesthetic such as 1% lidocaine with epinephrine (Fig. 43-4, step 1). Delay the incision for more than 30 seconds after infiltration of local anesthetic to permit local vasospasm, which minimizes bleeding of the wound during the procedure. Semi-open Technique: Make a skin incision 4 to 6 cm in length with a No. 11 scalpel blade. Using Army-Navy retractors, proceed with blunt dissection to expose the rectus fascia (Fig. 43-4, steps 2 and 3). With the infraumbilical incision in the midline, continue blunt dissection until the linea alba is seen. Its crossing bands of crural fibers may be apparent.61 Make a small 2- to 3-mm opening in the linea alba with a No. 15 scalpel blade (Fig. 43-4, step 4). You may notice a tough, gritty sensation when cutting the linea alba with the scalpel. Place towel clips through this opening to grasp each side of the rectus fascia (Fig. 43-4, step 5). Ask an assistant to lift the two towel clips and carefully advance the catheter and trocar in a 45- to 60-degree caudad orientation. Proceed through the peritoneum into the peritoneal cavity (see Fig. 43-4, steps 6 and 7).62 Closed Technique: For the closed technique, introduce the catheter into the peritoneal space in a blind percutaneous fashion.63 Use the simple Seldinger (guidewire) method, in which a small-gauge guide needle is inserted into the peritoneal cavity in the midline just inferior to the umbilicus (Fig. 43-5, step 2). Pass a flexible wire through the needle (Fig. 43-5, step 3), and remove the needle but not the wire. Advance a soft catheter over the wire and into the peritoneal cavity. Make a small stab with a No. 11 scalpel blade at the entry site of the wire to allow easier passage of the catheter through the abdominal wall (Fig. 43-5, step 4). Rotate the catheter while pushing it over the guidewire to facilitate entry into the peritoneal cavity. Place the catheter into the right or left pelvic gutter. Always control the guidewire to avert intraabdominal migration of the wire. Withdraw the wire and aspirate for blood with a 10-mL syringe. Follow this with peritoneal lavage when necessary. Proponents of the guidewire technique promote its ease and rapidity.64–68 Those who prefer the semi-open method argue that the time until peritoneal aspiration, the more critical interval, is minimally different and that this method may have fewer complications and thus be more accurate than the guidewire technique.69–73 Note that for both the semi-open and closed approaches, the time until aspiration is performed should be no more than 2 to 5 minutes. The optimum location for DPL is at the infraumbilical ring at the inferior border of the umbilicus (Table 43-6). Here, between the rectus abdominis muscles there is adherence of the peritoneum and relative lack of vascularity and preperitoneal fat.61 Closed DPL should always be conducted here. In the event of second- or third-trimester pregnancy, a suprauterine approach is used. If midline scarring is present, a fully open technique at the lateral border of the rectus abdominis in the left lower quadrant may be necessary. The left side is preferred to avoid later confusion about whether an appendectomy has been performed. It is interesting to note that Moore and associates found no increase in complications or misclassified lavage when the closed technique was used in a small series of patients with previous abdominal surgery.74 In the presence of a pelvic fracture, use a fully open supraumbilical approach. This greatly decreases the likelihood of passing the catheter through a retroperitoneal hematoma that has dissected from the fracture anteriorly and across the abdominal wall.75 In patients with penetrating trauma, do not perform DPL through the stab or missile entry site. This approach can contaminate the intraperitoneal cavity, potentially exacerbate the abdominal wall bleeding, and lead to a false-positive result. TABLE 43-6 C, closed; DPL, diagnostic peritoneal lavage; FO, fully open; SO, semi-open. Once the catheter has been placed successfully into the peritoneal cavity, attach the right-angle adapter, extension tubing, and a non–Luer-Lok syringe and attempt aspiration (see Fig. 43-4, step 8). If 10 mm of blood is aspirated, the test is positive and the procedure is terminated. With penetrating trauma, acquisition of lesser amounts may be meaningful because of the tendency for the diaphragm and bowel to hemorrhage minimally when injured. However, no rules have been established in this regard. If little to no blood is aspirated, lavage the peritoneal cavity with either normal saline or lactated Ringer’s solution (see Fig. 43-4, step 9). Apply a blood pressure cuff or blood infusion pump around the plastic intravenous (IV) bag to speed the influx (i.e., decrease lavage time) if necessary. Large-bore infusion tubing (e.g., urologic irrigation tubing sets, such as the Abbott No. 6543 cystoscopy/irrigation set) also shortens fluid influx time. Infuse 1 L of fluid in adults or 15 mL/kg in children. When possible, roll or shift the patient from side to side after the infusion to increase mixing. Place the IV bag or bottle on the floor (or below abdominal level), and allow the fluid to return by gravity. Return of 700 mL or more in an adult is generally accepted as adequate for interpretation of the findings. However, as little as 10% to 20% of the infusate may give a representative sample for both gross and microscopic determination. Send 10 mL of fluid from the return to the laboratory for cell count analysis, and send another 10 mL for enzyme analysis (see the section “Interpretation” later in this chapter). Some operators prefer to leave the catheter in place until the returned fluid is analyzed so that lavage may be repeated if the initial results are borderline or an occult bowel perforation is suspected. Local wound complications, including infection, hematoma, and dehiscence, occurred in only 0.3% of patients in two large series.42,76 Dehiscence with evisceration is an even rarer condition.77 Systemic infection has been described rarely (Table 43-7). Inability to recover peritoneal aspirate or lavage fluid can result in a false-negative interpretation. This can occur in several circumstances. It follows unwitting placement of the catheter into the preperitoneal space, which is less likely to occur with either open technique. Compartmentalization of fluid by adhesions or obstructing omentum can impede the egress of fluid. When a fully open supraumbilical or suprauterine technique is used, the catheter may be too short to access the depths of the intraperitoneal cavity. Finally, the large diaphragmatic tears typical of blunt pathophysiology allow flow of lavage fluid from the intraperitoneal to the thoracic cavity. Saunders and coworkers compared percutaneous DPL and the open technique in a prospective, randomized trial.78 Fluid obtained by the two techniques had similar test performance for intraabdominal pathology. The open technique took, on average, more than 4 minutes longer, but the percutaneous approach had an 11.2% technical failure rate (versus 3.8% with the open approach). False-positive findings can occur in two ways. First, iatrogenic misadventure may be responsible. Second, in penetrating trauma, particularly stab wounds, bleeding from the abdominal wall injury site into the peritoneal cavity can lead to positive findings when no injury to intraperitoneal structures has occurred.44 Recovery of 10 mL or more of blood via aspiration is considered a positive finding. Aspirates with lesser volume are generally discarded and are not factored into analysis of the lavage fluid. Grossly bloody aspirates are typically indicative of solid visceral or vascular injury, with a positive predictive value of greater than 90%.79,80 Aspiration of blood is responsible for approximately 80% of true-positive DPL findings with blunt trauma and for 50% with stab wounds.43 A positive aspiration in a blunt trauma patient who is hemodynamically stable or has been resuscitated to apparent stability need not mandate urgent surgery. Unnecessary laparotomy will occur if there has been minimal and self-limited damage to the liver, spleen, bowel serosa, or mesentery.81 In this situation, CT and clinical indicators should be used in concert with the findings on DPL. The recommended red blood cell (RBC) threshold varies according to the mechanism and, in the case of stab wounds, the external site of injury (Table 43-8). The optimum criterion will deliver excellent sensitivity, a high positive predictive value, and a minimal incidence of unnecessary laparotomy. Negative laparotomy incurs a prolongation of hospitalization and increases the cost of care, in addition to creating the potential for procedural complications.82,83 RBC counts greater than 105/mm3 (105/µL) are generally considered positive with a blunt mechanism or after stab wounds in the anterior part of the abdomen, flank, or back. Counts of 20,000 to 100,000/mm3 should be considered indeterminate.43,45,84,85 For stab wounds in the low chest region, where the diaphragm is at increased risk for injury, the RBC criterion should be lowered to 5000/mm3 to maximize sensitivity for isolated injury to this structure.36,43,86,87 With gunshot wounds involving the abdomen or low chest region, the same RBC criterion of 5000/mm3 is applied. This is intended to increase the sensitivity of the test because intraperitoneal entry by a missile carries a 90% or greater likelihood of intraperitoneal injury.36,60,88 An uncomplicated DPL should not result in more than several hundred to several thousand RBCs in the peritoneal lavage fluid. TABLE 43-8 Diagnostic Peritoneal Lavage RBC Criteria (per mm3) *In a hemodynamically stable patient with a pelvic fracture and a positive or equivocal red blood cell count, computed tomography should be obtained to corroborate or refute intraperitoneal injury. From Marx J, Isenhour J. Abdominal trauma. In: Marx JA, Hockberger RS, Walls RM, et al, eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 6th ed. St. Louis: Mosby; 2006:500.
Peritoneal Procedures
DPL
Indications
MANIFESTATION
PITFALL
Unstable vital signs with strongly suspected abdominal injury
Alternative sources of shock
Unequivocal peritoneal irritation
Unreliable
Pneumoperitoneum
Insensitive; may be due to a cardiopulmonary source or invasive procedures (diagnostic peritoneal lavage, laparoscopy)
Evidence of diaphragmatic injury
Nonspecific
Significant gastrointestinal bleeding
Uncommon, unknown accuracy
Penetrating Trauma
MANIFESTATION
PREMISE
PITFALL
Hemodynamic instability
Major solid visceral or vascular injury
Thorax, mediastinum
Peritoneal signs
Intraperitoneal injury
Unreliable, especially immediately after injury
Evisceration
Additional bowel, other injury
No injury in one fourth to one third of stab wound cases
Diaphragmatic injury
Diaphragmatic herniation
Rare clinical, radiographic findings
Gastrointestinal and vaginal hemorrhage
Proximal gut or uterine injury
Uncommon, unknown accuracy
Impalement in situ
Vascular impalement
High operative risk, pregnancy
Intraperitoneal air
Perforation of a hollow viscus
Insensitive; may be caused by intraperitoneal entry only or be due to a cardiopulmonary source
Procedure
Placement of the Catheter
Site
CLINICAL CIRCUMSTANCE
SITE
METHOD
Standard adult
Infraumbilical midline
C or SO
Standard pediatric
Infraumbilical midline
C or SO
Second- and third-trimester pregnancy
Suprauterine
FO
Midline scarring
Left lower quadrant
FO
Pelvic fracture
Supraumbilical
FO
Penetrating trauma
Infraumbilical midline*
C or SO
Aspiration and Lavage
Complications
Technical Failure
Interpretation
RBC Count
POSITIVE
INDETERMINATE
Blunt trauma
100,000*
20,000-100,000
Stab wound
Anterior abdomen
100,000
20,000-100,000
Flank
100,000
20,000-100,000
Back
100,000
20,000-100,000
Low chest
5000-10,000
1000-5000
Gunshot wound
5000-10,000
1000-5000
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Peritoneal Procedures
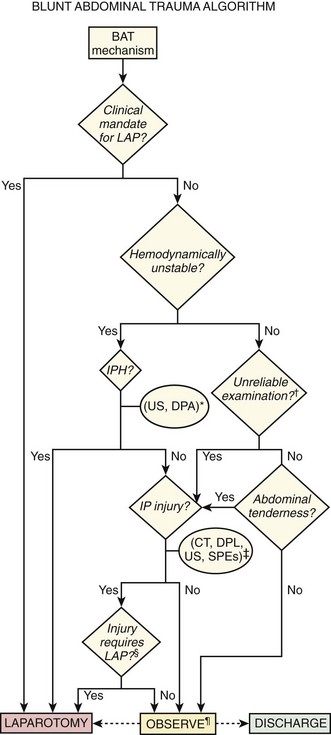
 The duration of observation should be 6 to 24 hours, depending on whether diagnostic tests have been performed, the results of the tests, and clinical circumstances, including the absence of factors rendering the examination unreliable. CT, computed tomography; D/C, discharge; DPA, diagnostic peritoneal aspiration; DPL, diagnostic peritoneal lavage; IP, intraperitoneal; IPH, intraperitoneal hemorrhage; LAP, laparotomy; SPE, serial physical examination; US, ultrasound.
The duration of observation should be 6 to 24 hours, depending on whether diagnostic tests have been performed, the results of the tests, and clinical circumstances, including the absence of factors rendering the examination unreliable. CT, computed tomography; D/C, discharge; DPA, diagnostic peritoneal aspiration; DPL, diagnostic peritoneal lavage; IP, intraperitoneal; IPH, intraperitoneal hemorrhage; LAP, laparotomy; SPE, serial physical examination; US, ultrasound. 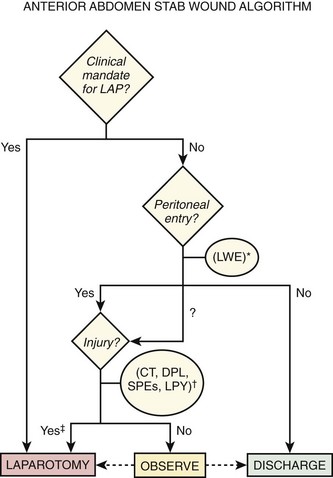
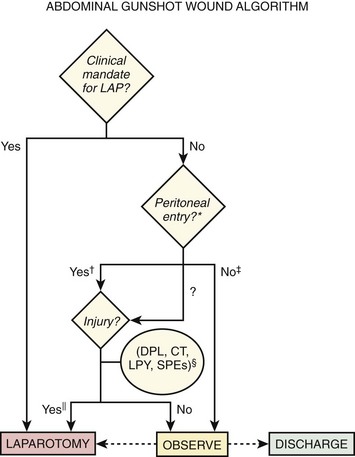
 Expectant management of injuries caused by gunshot wounds is rarely attempted. CT, computed tomography; D/C, discharge; DPL, diagnostic peritoneal lavage; LAP, laparotomy; LPY, laparoscopy; SPE, serial physical examination.
Expectant management of injuries caused by gunshot wounds is rarely attempted. CT, computed tomography; D/C, discharge; DPL, diagnostic peritoneal lavage; LAP, laparotomy; LPY, laparoscopy; SPE, serial physical examination.