Chapter 8 THE PELVIS
Clinically, the pelvis is an important region as it contains the rectum, anal sacs, prostate and male accessory organs, female reproductive tract and part of the urinary tract. For the purposes of this chapter, we have placed the reproductive tracts and urinary tract together in the pelvis.
In cases of trauma and road traffic accidents complete penile removal may be required.





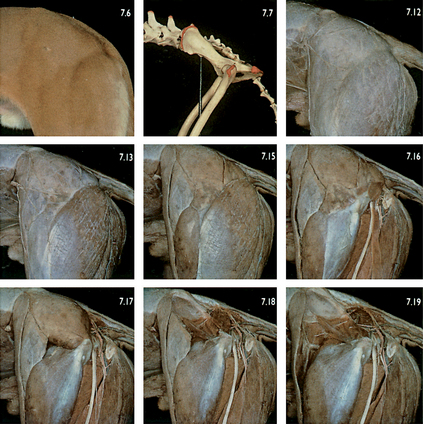
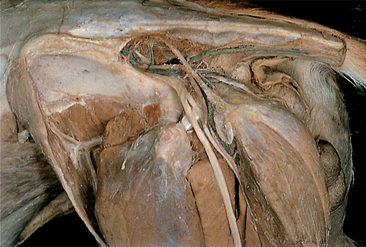
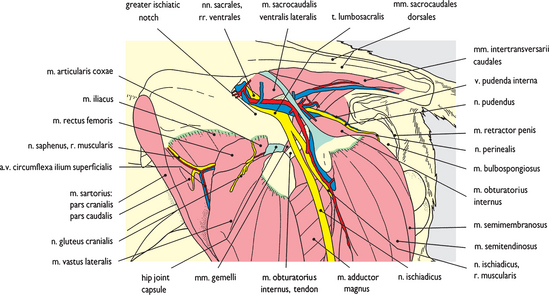
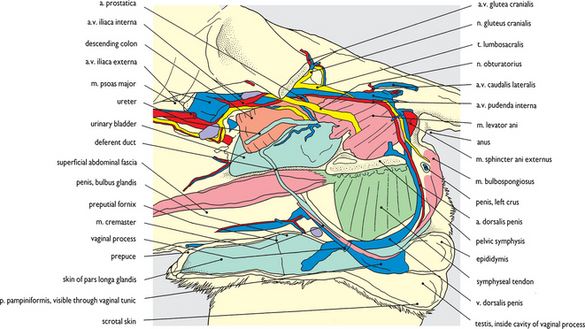
Fig. 8.9 Pelvic cavity and sacrotuberous ligament: left dorsolateral view. This is a slightly different view of Fig. 7.20, looking down into the pelvis through the greater ischiatic notch and onto the hip joint. The lumbosacral trunk is clearly exposed in this view leaving the pelvis to be continued as the ischiatic nerve. Caudal to the sacrotuberous ligament the coccygeal muscle and the external anal sphincter muscle form the medial boundary of the ischiorectal fossa (see Fig. 8.66). The internal obturator muscle forming the floor and lateral wall of the fossa leaves the pelvis and its tendon is visible on the gemelli muscles beneath the ischiatic nerve. Immediately cranial to it the hip joint capsule has been exposed and the articularis coxae muscle lies on its surface. The retractor penis muscle and the bulbospongiosus muscle are both exposed on the root of the penis (see Fig. 8.44).
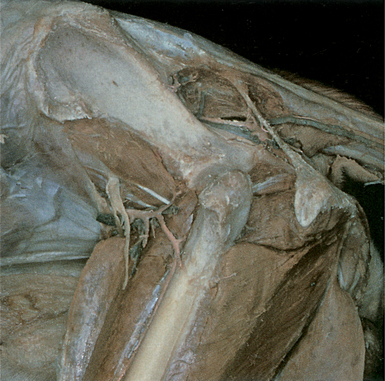
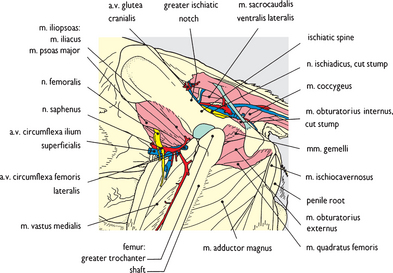


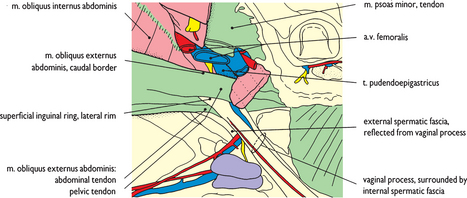
Fig. 8.13 Inguinal canal (1). External abdominal oblique muscle and superficial inguinal ring: left lateral view. This is a closer view of the inguinal region of a dog and begins a sequence of inguinal canal dissections (see Figs 8.53–8.57 for a ventral sequence in a bitch). Abdominal fascia has been cleared to expose the superficial inguinal ring, and reflection of spermatic fascia has exposed the vaginal process. The femoral vessels are cut back to expose the caudal border of the external oblique muscle.

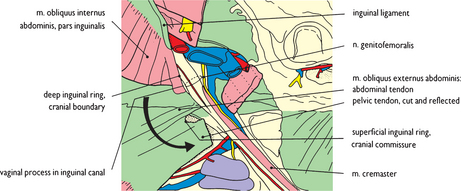

Fig. 8.15 Inguinal canal (3). Internal abdominal oblique muscle, spermatic fascia and cremaster muscle: left lateral view. The reflected part of the external oblique has been removed and the line of the cut edge of the tendon is visible on the rectus abdominis muscle where it contributes to the rectus sheath (see Chapter 6). The approximate positions of the inguinal rings, and therefore the extent of the inguinal canal, are shown.

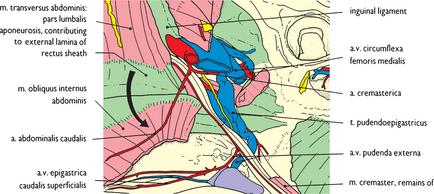

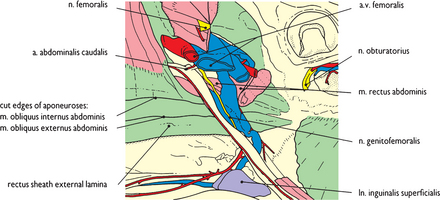

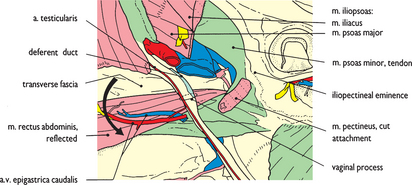
Fig. 8.18 Inguinal canal (6). Vaginal process, testicular artery and deferent duct: left lateral view. The transverse abdominal muscle has been cut through on a line with the dorsal edge of the rectus abdominis allowing the rectus to be reflected ventrally away from the abdominal wall, totally destroying what remains of the inguinal canal. Transverse fascia lines the abdomen and here forms the internal layer of the rectus sheath (see Chapter 6).
< div class='tao-gold-member'>