Patrick M. McCue
Ovarian Abnormalities
Ovarian abnormalities may arise from transient pathophysiologic conditions, such as a luteinized anovulatory follicle, or may be associated with more permanent pathologic issues, such as a granulosa cell tumor. Some ovarian issues are commonly identified in clinical practice, whereas others are diagnosed very infrequently (Box 161-1). Diagnosis is usually made on the basis of a combination of behavioral observations, by palpation and ultrasonography per rectum, and potentially by hormone analysis. Additional tests such as ovarian biopsy and karyotyping can be important diagnostic tests in some cases.
Failure of Follicular Development
Alterations of follicular development may be associated with a variety of physiologic and pathologic conditions.
Ovarian Senescence
Ovarian dysfunction has been identified as a cause of reduced fertility in mares approximately 20 years of age or older. These older mares may have a longer follicular phase, prolonged interovulatory period, and delay in first ovulation of the year. Complete failure of follicular development or ovarian senescence, which occurs in some aged mares, may be a result of an insufficient number of primordial follicles. Ultrasound examination will reveal ovaries that contain only small (i.e., <10 to 15 mm) follicles and no luteal structures over a prolonged period of time during the physiologic breeding season. No effective treatments are available to promote follicular growth in senescent ovaries.
Postpartum Anestrus
Most mares develop follicles and ovulate early in the postpartum period (i.e., the foal heat ovulation) and continue to cycle if they are not bred or do not become pregnant. However, some mares may have temporary failure of follicular development or ovulation after foaling. Affected mares may remain anovulatory or in anestrus for weeks or months before cyclic ovarian activity begins again. Mares that foal early in the year are more prone to have postpartum anestrus than mares foaling later in the spring or in the summer. This postpartum anestrus may be caused by the combined effects of season, nutrition, and lactation. Administration of recombinant equine follicle-stimulating hormone (reFSH, 0.65 mg, IM, every 12 hours) will stimulate follicular development within 7 to 10 days; administration of human chorionic gonadotropin (hCG, 1500 to 2500 units, IV or IM) is required to induce ovulation.
Exogenous Hormone Treatment
Administration of anabolic steroids, dexamethasone, estradiol esters, and a combination of progesterone plus estradiol have all been reported to suppress pituitary gonadotropin secretion and ultimately result in inhibition of ovarian follicular activity. Potent agonists of gonadotropin-releasing hormone (GnRH), such as deslorelin acetate, cause downregulation of pituitary gonadotropin secretion and short-term alterations in ovarian function.
Gonadotropin-Releasing Hormone Vaccine Administration
Active immunization of mares against GnRH may be performed to keep mares out of heat for a prolonged period of time. Immunization results in suppression of pituitary FSH and luteinizing hormone (LH) secretion and a subsequent reduction in ovarian follicular activity, suppression of estrus, and decreased fertility that is related to the magnitude and duration of antibody titer. In most instances, the effect is reversible over time as antibody titers wane, and vaccinated mares eventually resume ovarian function and return to normal fertility. However, some mares immunized against GnRH fail to return to cyclicity even after several years.
Anovulatory Follicles
Approximately 8% of large dominant estrual follicles fail to ovulate during the physiologic breeding season in mares. Most (85%) anovulatory follicles become hemorrhagic and eventually luteinize, whereas about 15% of anovulatory follicles do not become hemorrhagic and remain as persistent anovulatory follicles.
Persistent Anovulatory Follicles
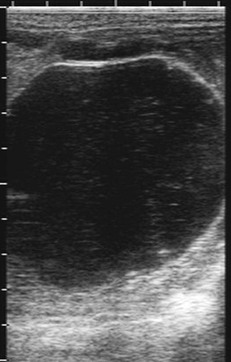
Persistent anovulatory follicles are not associated with significant hemorrhage or luteinization, and serum progesterone concentrations are less than 1.0 ng/mL. Persistent anovulatory follicles are recognized on ultrasonographic examination as large static follicular structures with few to no echogenic particles or strands within the lumen (Figure 161-1). Affected mares go out of heat and endometrial edema declines as estradiol levels decrease. After several weeks, these nonluteinized anovulatory follicles eventually regress or undergo atresia, and they are eventually replaced by another dominant follicle.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


