Chapter 17 Orbit
ANATOMY
The orbit is the cavity that encloses the eye. The two orbital patterns in domestic animals are as follows:
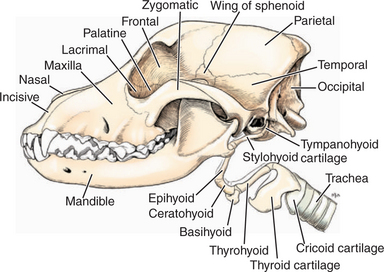
Figure 17-1 Bones of the skull, hyoid apparatus, and laryngeal cartilages, lateral aspect.
(Modified from Evans HE [1993]: Miller’s Anatomy of the Dog, 3rd ed. Saunders, Philadelphia.)
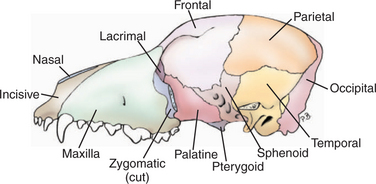
Figure 17-2 Skull, lateral aspect (zygomatic arch removed).
(Modified from Evans HE [1993]: Miller’s Anatomy of the Dog, 3rd ed. Saunders, Philadelphia.)
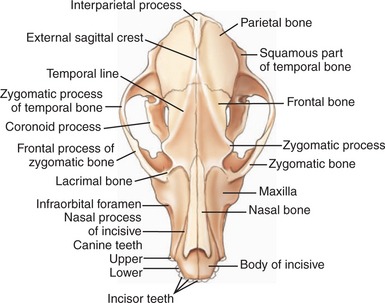
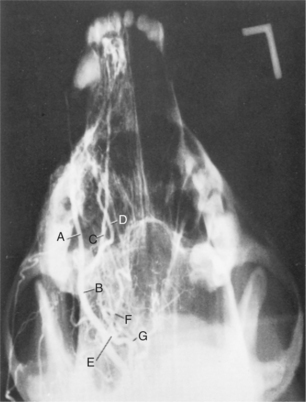
Figure 17-3 Dorsal view of the canine skull.
(Modified from Getty R [1975]: Sisson and Grossman’s the Anatomy of the Domestic Animals, 5th ed. Saunders, Philadelphia.)
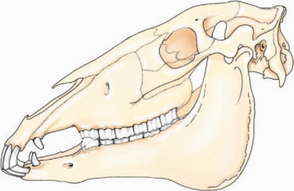
Figure 17-4 Left lateral view of the equine skull. Note the enclosed dorsolateral surface of the orbit.
(Modified from Dyce KM, et al. [2002]: Textbook of Veterinary Anatomy, 3rd ed. Saunders, Philadelphia.)
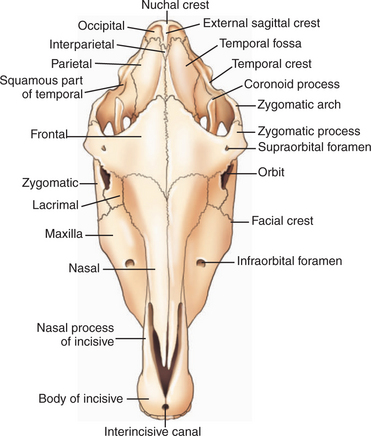
Figure 17-5 Dorsal view of the equine skull.
(Modified from Getty R [1975]: Sisson and Grossman’s the Anatomy of the Domestic Animals, 5th ed. Saunders, Philadelphia.)
The orbit separates the eye from the cranial cavity, and the foramina and fissures in its walls determine the path of blood vessels and nerves from the brain to the eye. The walls of the equine orbit are formed by the frontal, lacrimal, zygomatic, temporal, presphenoid, palatine, and maxillary bones, which are similar in other species. In the dog and cat the dorsolateral portion of the orbit is spanned by the dense collagenous orbital ligament, which passes from the zygomatic process of the frontal bone to the frontal process of the zygomatic bone. The basic foramina and fissures of the orbit are the orbital, rostral and caudal alar, oval, supraorbital, ethmoidal, lacrimal, maxillary, sphenopalatine, round, and palatine. In cattle, the orbital foramen and the foramen rotundum fuse to form the foramen orbitorotundum. The vessels and nerves that pass through these foramina and fissures in the dog are shown in Figures 1-16, 1-17, and 1-19 to 1-22 in Chapter 1 and Figure 17-6.
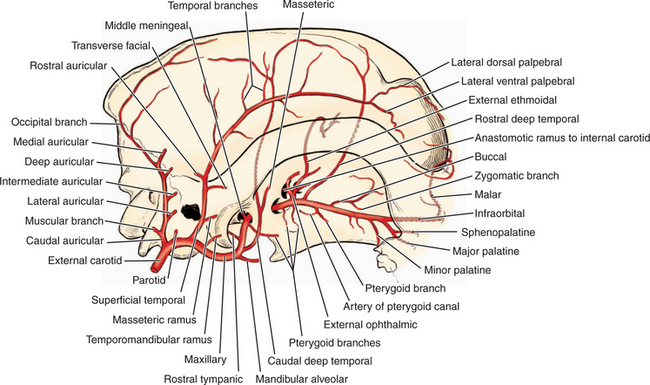
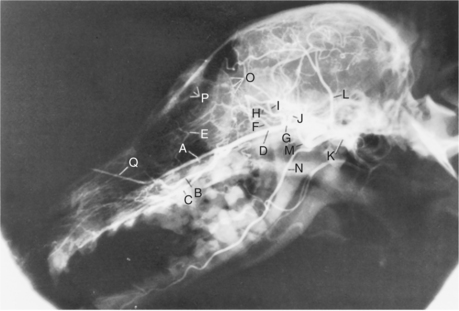
Figure 17-6 Arteries of the head in relation to lateral aspect of the skull.
(Modified from Evans HE [1993]: Miller’s Anatomy of the Dog, 3rd ed. Saunders, Philadelphia.)
The position of the orbit within the skull varies with species. In cattle, sheep, and horses the eyes are situated laterally, giving panoramic vision, whereas in dogs and cats the eyes are located more anteriorly, which emphasizes binocular overlap between the two eyes. The visual, orbital, and optic axes, defined as follows, do not coincide (Figure 17-7):
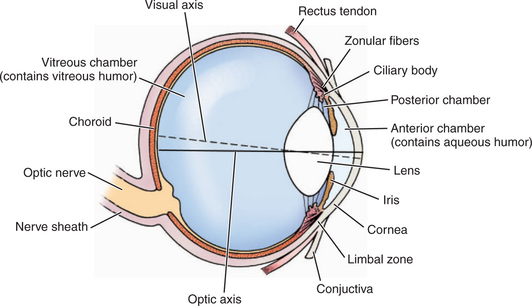
Figure 17-7 The visual and optic axes of the eye.
(Modified from Getty R [1975]: Sisson and Grossman’s the Anatomy of the Domestic Animals, 5th ed. Saunders, Philadelphia.)
The angle formed by the optic axes, a measure of binoc-ular overlap, is shown in different species in Figures 17-8 to 17-10.
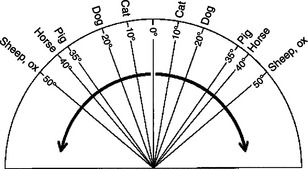
Figure 17-8 Comparison of the angle formed by the optic axes of different species of domestic animals.
(From Getty R [1975]: Sisson and Grossman’s the Anatomy of the Domestic Animals, 5th ed. Saunders, Philadelphia.)
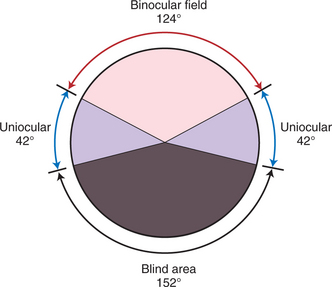
Figure 17-9 Visual field of a primate, showing a large binocular field, small uniocular areas, and a large blind area.
(Modified from Duke-Elder S [1958]: System of Ophthalmology, Vol I: The Eye in Evolution. H. Compton, London.)
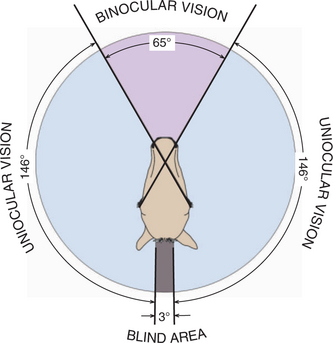
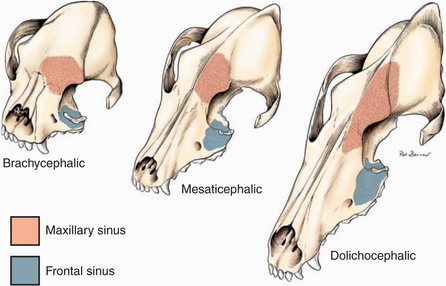
Figure 17-11 Relationship of the paranasal sinuses to the orbital walls in the dog.
(Modified from Evans HE [1993]: Miller’s Anatomy of the Dog, 3rd ed. Saunders, Philadelphia.)

The orbital contents are completely enclosed in a sheet of connective tissue—the periorbita—that lies next to the bone in the bony parts of the orbital wall and that is thicker laterally where the wall is incomplete (in carnivores). The periorbita is reflected over the extraocular muscles and forward over the globe to become Tenon’s capsule, lying beneath the conjunctiva (Figure 17-14). The periorbita is continuous with the periosteum of the facial bones at the orbital rim, with the orbital septum anteriorly, and with the dura mater of the optic nerve. The orbital fat pad lies between the periorbita and the extraocular muscles. Intraorbital fat lies between the muscles and fascial layers (Figure 17-15). In animals with an incomplete bony orbit, the masticatory muscles play a critical role in providing posterior support for the orbital contents. Orbital disease processes may thus be located in one of the following three planes:
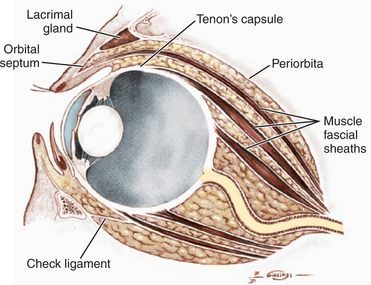

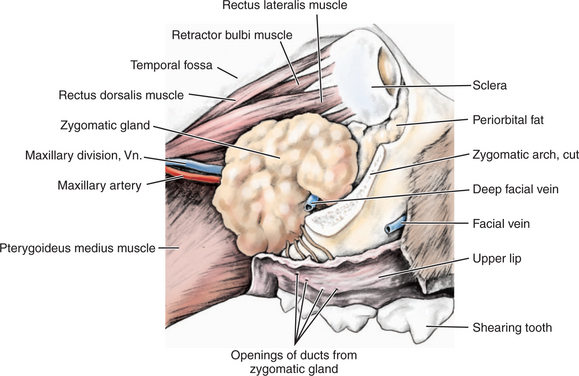
The lacrimal gland lies beneath the orbital ligament on the dorsolateral surface of the globe (see Figure 17-14). The base of the third eyelid and gland is held down by the orbital retinaculum, which are poorly defined sheets of collagenous tissue continuous with the periorbita but that contain smooth muscle with sympathetic innervation.
Extraocular Muscles
Seven extraocular muscles control movements of the globe (Figure 17-16; Table 17-1). The extraocular muscles arise from the annulus of Zinn, which circles the optic foramen and orbital fissure, and insert onto the globe. Neurologic abnormalities in their function are discussed in Chapter 16.
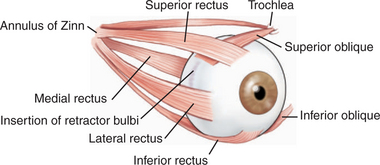
Figure 17-16 General arrangement of the orbital muscles.
(Modified from Prince JH, et al. [1960]: Anatomy and Histology of the Eye and Orbit in Domestic Animals. Charles C. Thomas, Springfield, IL.)
Table 17-1 Extraocular Muscles: Actions and Innervations
| MUSCLE | INNERVATION | ACTION |
|---|---|---|
| Superior (dorsal) rectus | Oculomotor (CN III) | Elevates globe |
| Inferior (ventral) rectus | Oculomotor (CN III) | Depresses globe |
| Medial rectus | Oculomotor (CN III) | Turns globe nasally |
| Lateral rectus | Abducens (CN VI) | Turns globe temporally |
| Superior (dorsal) oblique | Trochlear (CN IV) | Intorts globe (rotates 12 o’clock position nasally) |
| Inferior (ventral) oblique | Oculomotor (CN III) | Extorts globe (rotates 12 o’clock position temporally) |
| Retractor bulbi | Abducens (CN VI) | Retracts globe |
| Levator superioris | Oculomotor (CN III) | Elevates upper lid |
CN, Cranial nerve.
PATHOLOGIC MECHANISMS
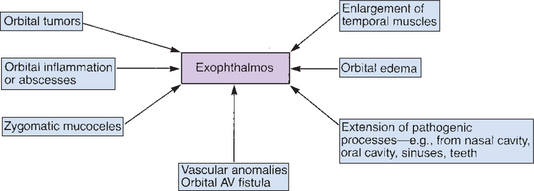
Because the orbit forms a semiclosed space, increases and decreases in the volume of its contents affect the position of the eye in relation to the orbital rim and to the other eye. Space-occupying lesions (Figure 17-17) push the eye forward, causing exophthalmos, and often the third eyelid also protrudes as it is passively forced out of the orbit. In dogs and cats orbital masses usually result in swelling of the tissues caudal to the last upper molar tooth, because the orbital floor is only soft tissue in this area. With decreased volume of the orbital contents (e.g., dehydration or atrophy of fat or muscle), the eye sinks further into the orbit—enophthalmos—and the third eyelid protrudes. Osteomyelitis of the bones forming the orbit due to organisms such as Cryptococcus and Actinomyces spp. may also cause exophthalmos.
The position of space-occupying lesions alters the direction of displacement of the globe and is used to determine the site of the offending mass (Figure 17-18) and the optimal route of surgical exploration.
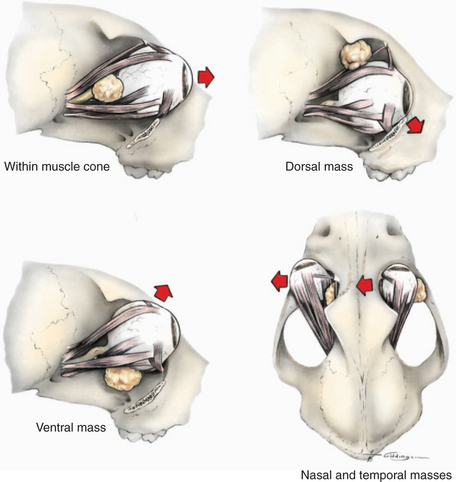
Figure 17-18 Effects of space-occupying lesions on the direction of globe displacement (as indicated by arrows).
Because of the many tissue types present, numerous kinds of neoplasms may affect the orbit. The most common causes of exophthalmos in one case series of dogs and cats were neoplasia (52%), orbital abscesses/cellulitis (30%), hematoma (9%), zygomatic mucocele (5%), arteriovenous fistula (2%), and eosinophilic myositis (2%).
DIAGNOSTIC METHODS
The diagnosis of orbital disorders requires a complete ophthalmic examination and perhaps additional special diagnostic techniques, as follows (Figure 17-19).
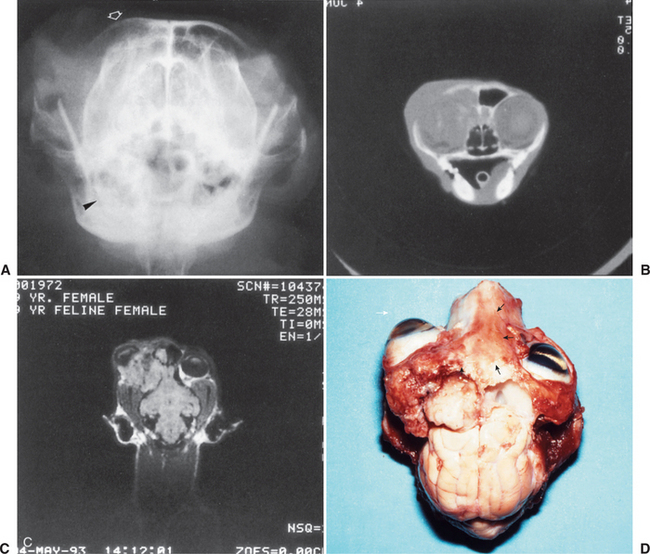

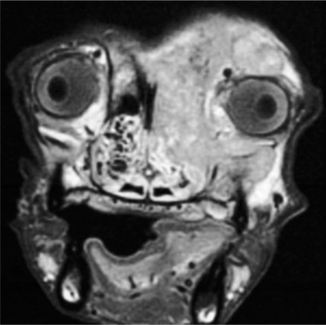
Figure 17-21 Magnetic resonance image of nasal carcinoma invading the orbit of a dog and causing exophthalmos.
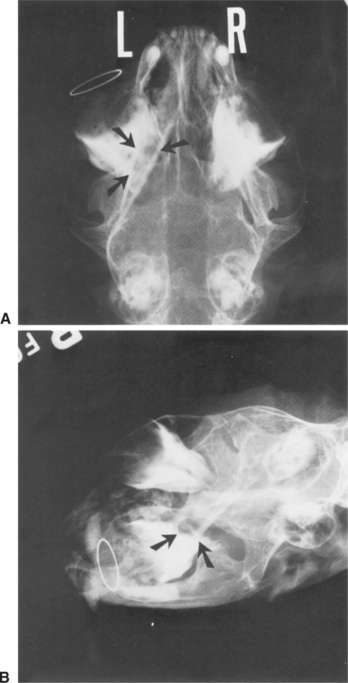
Localization of Foreign Bodies
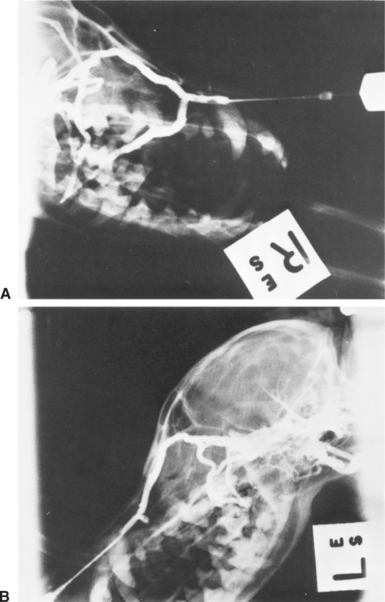
Depending on the type of foreign body, ultrasonography or radiography can be used to localize a foreign body. For radiography a reference ring of wire may be placed at the limbus (see Figure 17-23); radiographs are taken at four different angles (lateral, ventrodorsal, oblique, frontal) in an attempt to differentiate ocular and orbital foreign bodies and determine their location. Nonmetallic foreign bodies tend to be better visualized ultrasonographically. Porcupine quills, which are common orbital foreign bodies in dogs in certain geographic areas, have a characteristic double-banded, linear hyperechoic appearance useful in identifying, localizing, and establishing a prognosis. Wooden slivers, however, are not easily visualized with either technique.
ORBITAL DISEASES
A summary of orbital diseases, classified by type, is given in Table 17-2.
Table 17-2 Summary of Orbital Diseases
| TYPE OF DISORDER | CONDITION | CLINICAL SIGNS |
|---|---|---|
| Developmental abnormalities | ||
| Trauma | 1. Subconjunctival and episcleral hemorrhages; retrobulbar hemorrhage with exophthalmos or proptosis 2. Discharging sinus fluid through the conjunctiva, periocular skin, buccal mucosa; pain on opening mouth Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|