Chapter 3 THE NECK
The neck has three regions: the parotid region, the ventral margin of the neck and the prescapular region. Many conditions link the head and the neck and one of the most important is the brachycephalic dog that has upper airway syndrome due to distortion of the face.

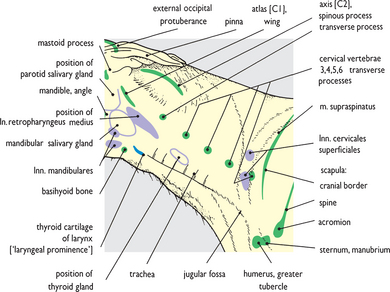
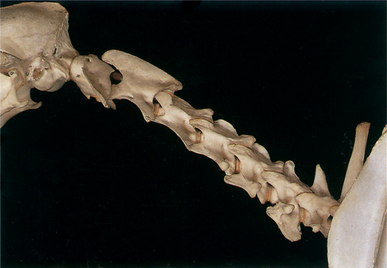
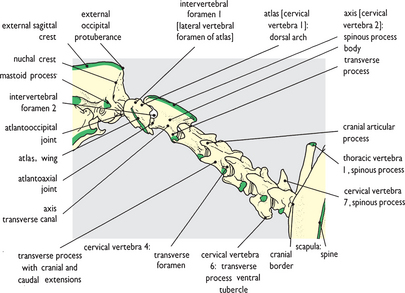
Fig. 3.2 Skeleton: left lateral view. The palpable bony features shown in Fig. 3.1 are colored green on this diagram for reference. However, any features of cervical vertebrae 3 to 7 are, even in thin dogs, only palpable with difficulty, and not at all in larger breeds.
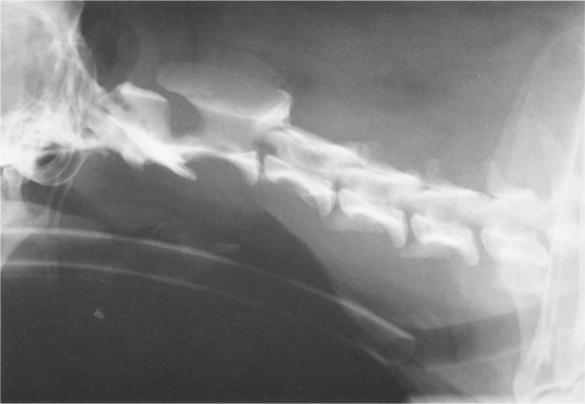
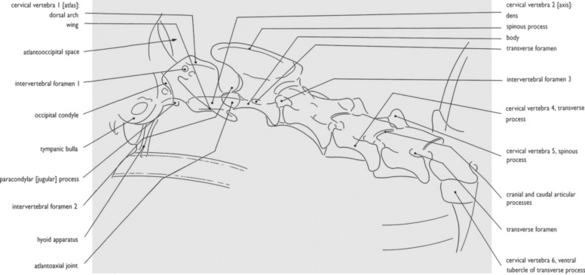

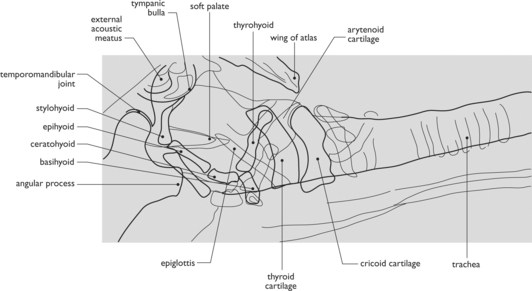

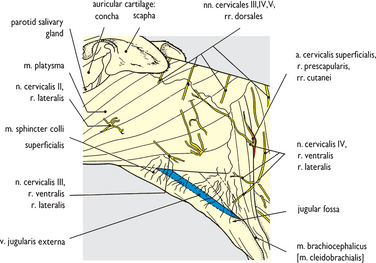


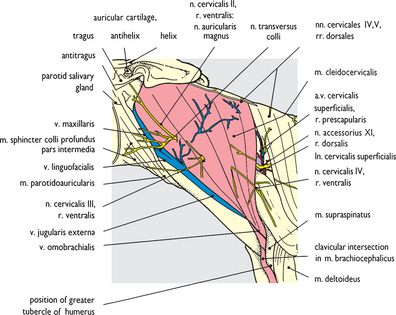
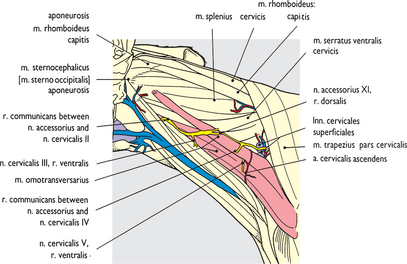
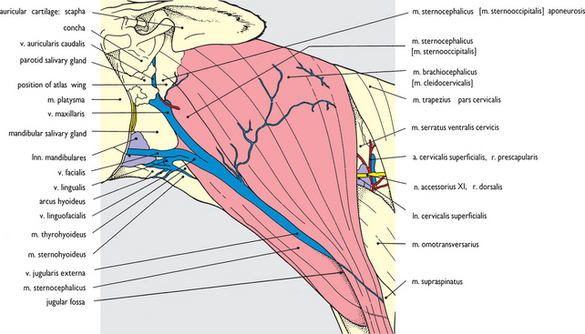
Fig. 3.8 Superficial structures (3). Cutaneous nerves and external jugular vein: left lateral view. The platysma muscle has been removed, and the superficial fascia cleared, to expose the underlying muscles, and isolate cutaneous ramifications of cervical nerves 2, 3 and 4. Cervical nerve 5 lacks lateral cutaneous branches, whilst cervical nerves 6, 7 and 8 contribute to the brachial plexus (see Fig. 3.19). Cutaneous branches from cervical nerve 4 distribute to the base of the neck.

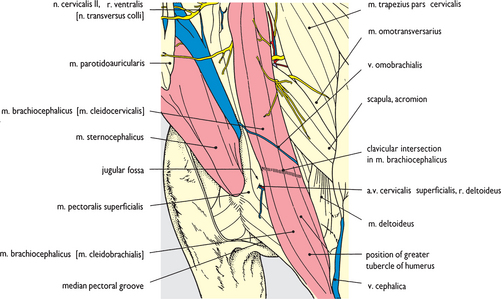
Fig. 3.9 Superficial structures (4). Cutaneous nerves, external jugular vein and jugular fossa: left craniolateral view. This clearly demonstrates the jugular fossa at the base of the neck and the deep and somewhat triangular depression bounded by sternocephalic, brachiocephalic and superficial pectoral muscles (see also Fig. 3.41). Also evident is the clavicular intersection within the brachiocephalic muscle, denoted by an indistinct fascial line lateral to the jugular fossa.

< div class='tao-gold-member'>