Chapter 7 Movement
Gait
 Depending on the part of the stride during which observations begin, the walk can appear to be lateral or diagonal. In general, in a lateral gait, both feet on one side strike the ground before the feet on the contralateral side. In a diagonal gait, one foot strike is followed by a strike of the foot located diagonal and contralateral to the initial foot (e.g., LF followed by the RH).
Depending on the part of the stride during which observations begin, the walk can appear to be lateral or diagonal. In general, in a lateral gait, both feet on one side strike the ground before the feet on the contralateral side. In a diagonal gait, one foot strike is followed by a strike of the foot located diagonal and contralateral to the initial foot (e.g., LF followed by the RH). Stride length should be evaluated and compared with observations at the trot. Stride length and sequence of footfalls are easier to see while horses are walking than while they are trotting. Horses with hindlimb lameness may be examined for failure to track up.5 Horses normally track up, or overtrack. The hind foot is placed in or in front of the imprint of the ipsilateral front foot. Failure to track up usually is caused by hindlimb lameness or poor impulsion, and the hind foot imprint is seen behind that of the ipsilateral front foot.5 Although unusual, occasionally a horse will be observed to pace while walking, a finding that may indicate the presence of neurological disease. In breeds unassociated with the pace or similar gaits, young horses that pace should undergo careful neurological evaluation. Pacing while walking may be completely normal, and in older, “made” horses (horses that have already achieved an upper level of performance) the finding should not be overinterpreted.
Stride length should be evaluated and compared with observations at the trot. Stride length and sequence of footfalls are easier to see while horses are walking than while they are trotting. Horses with hindlimb lameness may be examined for failure to track up.5 Horses normally track up, or overtrack. The hind foot is placed in or in front of the imprint of the ipsilateral front foot. Failure to track up usually is caused by hindlimb lameness or poor impulsion, and the hind foot imprint is seen behind that of the ipsilateral front foot.5 Although unusual, occasionally a horse will be observed to pace while walking, a finding that may indicate the presence of neurological disease. In breeds unassociated with the pace or similar gaits, young horses that pace should undergo careful neurological evaluation. Pacing while walking may be completely normal, and in older, “made” horses (horses that have already achieved an upper level of performance) the finding should not be overinterpreted. Horses seldom back naturally, but backing commonly is required of horses during performance events, while exiting from a trailer, or while driving. Backing is useful during lameness examination to evaluate certain gait deficits, such as those associated with shivers, stringhalt, and neurological disease.
Horses seldom back naturally, but backing commonly is required of horses during performance events, while exiting from a trailer, or while driving. Backing is useful during lameness examination to evaluate certain gait deficits, such as those associated with shivers, stringhalt, and neurological disease. 
 The trot is theoretically a symmetrical gait, meaning both “halves” (beats) of the stride are identical, and at low speed in a sound horse, symmetry is likely achieved. However, at speed, perfect balance and fine management of weight (of the shoes) are necessary for a trotter to be perfectly symmetrical. There is a moment of suspension between impact of each diagonal pair of limbs. Some elite dressage horses do not have a two-beat gait but show advanced diagonal placement. This means that the hindlimb of a diagonal pair of limbs lands first and therefore is the only limb bearing weight. Hindlimb lameness is present in a higher percentage of horses that perform at speed at the trot compared with galloping horses because of differences in weight distribution in the trot and gallop. Compensatory lameness develops in the diagonal paired limb. LF lameness predisposes to RH lameness. Interference between limbs is more common in horses that trot at speed when compared with those that gallop. Likewise, hindlimb lameness is relatively common in dressage horses.
The trot is theoretically a symmetrical gait, meaning both “halves” (beats) of the stride are identical, and at low speed in a sound horse, symmetry is likely achieved. However, at speed, perfect balance and fine management of weight (of the shoes) are necessary for a trotter to be perfectly symmetrical. There is a moment of suspension between impact of each diagonal pair of limbs. Some elite dressage horses do not have a two-beat gait but show advanced diagonal placement. This means that the hindlimb of a diagonal pair of limbs lands first and therefore is the only limb bearing weight. Hindlimb lameness is present in a higher percentage of horses that perform at speed at the trot compared with galloping horses because of differences in weight distribution in the trot and gallop. Compensatory lameness develops in the diagonal paired limb. LF lameness predisposes to RH lameness. Interference between limbs is more common in horses that trot at speed when compared with those that gallop. Likewise, hindlimb lameness is relatively common in dressage horses. Pacers also have a high percentage of hindlimb lameness, but compensatory lameness usually develops in the lateral paired limb. RH lameness predisposes to RF lameness.
Pacers also have a high percentage of hindlimb lameness, but compensatory lameness usually develops in the lateral paired limb. RH lameness predisposes to RF lameness. The stance phase of the stride is relatively longer at the walk than at the trot. The deep digital flexor tendon and the collateral ligaments of the distal interphalangeal joint are stressed maximally with extension of the distal interphalangeal joint. Thus with severe injuries of either structure lameness may be more severe at the walk than at the trot because of greater extension of the distal interphalangeal joint associated with the relatively long stance duration.5 Horses with hindlimb lameness characterized by a shortened caudal phase of the stride at the walk but shortened cranial phase at the trot often have upper limb lameness, such as that caused by pelvic fractures or osteoarthritis of the coxofemoral joint or from severe pain originating from the foot. In general, horses that have limb flight characteristics that differ between walk and trot should be evaluated carefully because in my experience they often have bona fide pain originating from the upper limb or are affected with an unusual mechanical or neuromuscular deficit.
The stance phase of the stride is relatively longer at the walk than at the trot. The deep digital flexor tendon and the collateral ligaments of the distal interphalangeal joint are stressed maximally with extension of the distal interphalangeal joint. Thus with severe injuries of either structure lameness may be more severe at the walk than at the trot because of greater extension of the distal interphalangeal joint associated with the relatively long stance duration.5 Horses with hindlimb lameness characterized by a shortened caudal phase of the stride at the walk but shortened cranial phase at the trot often have upper limb lameness, such as that caused by pelvic fractures or osteoarthritis of the coxofemoral joint or from severe pain originating from the foot. In general, horses that have limb flight characteristics that differ between walk and trot should be evaluated carefully because in my experience they often have bona fide pain originating from the upper limb or are affected with an unusual mechanical or neuromuscular deficit. .5 A horse may have to be trotted up and down many times. It is sometimes useful for the examiner to lead the horse to assess subtle forelimb lameness, because gait abnormalities may become more obvious.
.5 A horse may have to be trotted up and down many times. It is sometimes useful for the examiner to lead the horse to assess subtle forelimb lameness, because gait abnormalities may become more obvious.Determination, Grading, and Characterization of Lameness
2 Possibility of involvement of more than one limb and presence of compensatory (coexistent) lameness
Compensatory Lameness
 The horse may be lame in one limb while being circled in one direction and lame in the contralateral limb in the opposite direction.
The horse may be lame in one limb while being circled in one direction and lame in the contralateral limb in the opposite direction. 
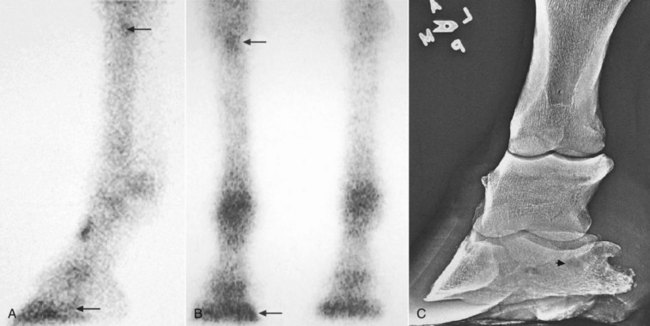
Compensatory lameness also can develop in the same limb. In horses with front foot lameness the suspensory ligament (SL) often is sore, and some horses have suspensory desmitis. In horses with lameness abolished by palmar digital analgesia, most with navicular syndrome, scintigraphic examination revealed increased radiopharmaceutical uptake (IRU) in the proximal palmar aspect of the McIII in 30% of horses, indicating possible abnormal loading of the proximal aspect of the SL (Figure 7-1).9 Complete resolution of lameness may not be achieved until high palmar analgesia is performed.
 In these horses, lameness is manifested in the swing phase of the stride with no apparent pain. Unfortunately, the term swinging limb lameness often is used inappropriately to describe the gait deficit in horses with painful, supporting limb lameness. Lameness associated with osteochondrosis of the scapulohumeral joint is often described as a swinging limb lameness because of a markedly shortened cranial phase of the stride. Dramatic improvement in the shortened cranial phase of the stride can be achieved by diagnostic analgesia, eliminating pain associated with lameness. Thus the gait deficit is the direct result of pain, and no clear differentiation between supporting and swinging limb lameness can be made. Horses with painful forelimb lameness almost always shorten the cranial phase of the stride, although perhaps not to the extreme as in a horse with authentic scapulohumeral joint lameness.
In these horses, lameness is manifested in the swing phase of the stride with no apparent pain. Unfortunately, the term swinging limb lameness often is used inappropriately to describe the gait deficit in horses with painful, supporting limb lameness. Lameness associated with osteochondrosis of the scapulohumeral joint is often described as a swinging limb lameness because of a markedly shortened cranial phase of the stride. Dramatic improvement in the shortened cranial phase of the stride can be achieved by diagnostic analgesia, eliminating pain associated with lameness. Thus the gait deficit is the direct result of pain, and no clear differentiation between supporting and swinging limb lameness can be made. Horses with painful forelimb lameness almost always shorten the cranial phase of the stride, although perhaps not to the extreme as in a horse with authentic scapulohumeral joint lameness.  Horses with any painful hindlimb lameness consistently shorten the cranial phase of the stride, a reliable clinical indicator of which limb is affected, and when pain is abolished, the cranial phase (swing phase) of the stride improves (lengthens). Because the terminology is confusing and often erroneous, I prefer to avoid use of these terms and simply describe lameness as accurately as possible. For instance, describing a horse as grade 2 of 5 LF lame, with a marked shortening of the cranial phase of the stride reminiscent of other horses I have seen with shoulder region lameness, gives the most accurate and useful information.
Horses with any painful hindlimb lameness consistently shorten the cranial phase of the stride, a reliable clinical indicator of which limb is affected, and when pain is abolished, the cranial phase (swing phase) of the stride improves (lengthens). Because the terminology is confusing and often erroneous, I prefer to avoid use of these terms and simply describe lameness as accurately as possible. For instance, describing a horse as grade 2 of 5 LF lame, with a marked shortening of the cranial phase of the stride reminiscent of other horses I have seen with shoulder region lameness, gives the most accurate and useful information.


