CHAPTER 14

Medical Records Management
Mastery of the content in this chapter will enable the reader to:
• Explain methods used to file records.
• Identify a completed medical record.
• List the benefits of using labels for medical records.
• Explain how to purge medical records when needed.
• Define the advantages and disadvantages of computerized medical records.
• Develop and provide patient discharge instructions.
• Identify common abbreviations.
• Describe methods used to file radiographs.
• Clarify the importance of backing up computer systems on a daily basis.
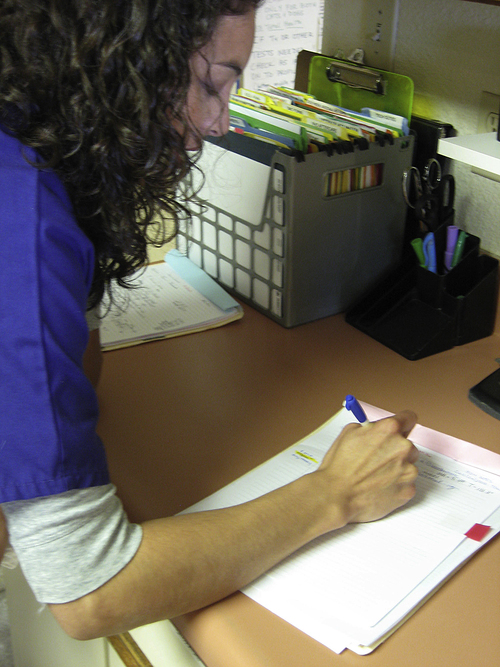
The office or practice manager should make it a daily task to pull random records and check for completeness. Practices get busy. The reception team takes the record to invoice the client, and occasionally it does not get returned to the original doctor or team member to be completed (Figure 14-1). Complete records must include the date of entry, initials of all team members writing in the record, a complete SOAP format, and all authorization forms a client has signed. If any charts have been referenced, those must also be in the record. The more information that is available in the medical record, the less the legal risk will be.
 PRACTICE POINT
PRACTICE POINTLEGIBILITY OF MEDICAL RECORDS
 PRACTICE POINT
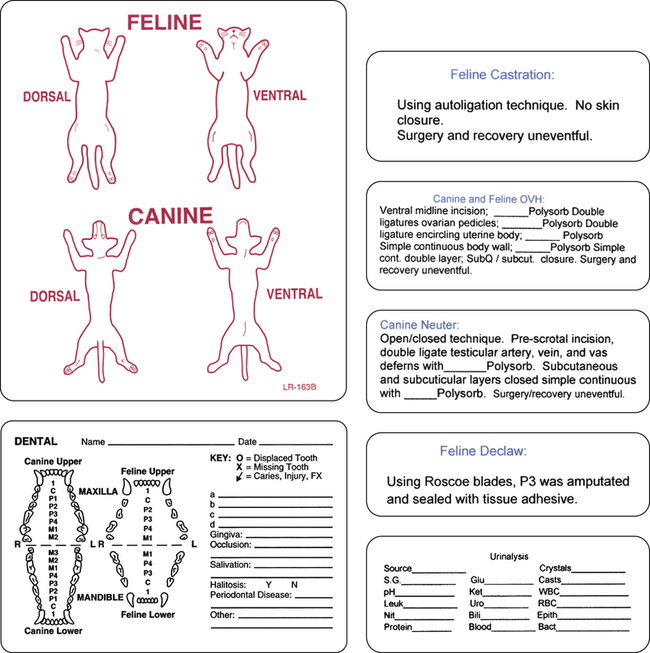
PRACTICE POINTIf legibility is problem within a veterinary practice, the use of labels or stamps may be suggested for routine procedures. Physical exams, urinalyses, routine dentals, and alterations are just a few labels that can be generated in a fill-in-the-blank form to accommodate details. Size of suture material can be easily added on surgical stickers, normal findings can be easily marked on physical exam stickers, and abnormal findings can be clearly defined below the label or stamp (Figure 14-2).
A medical record is a legal document. Correction fluid cannot be used on any medical record, release, or authorization form at any time. If a mistake needs to be corrected, a one-line strike-through can be written, with the author’s initials indicating the correction (Box 14-1).
CHOOSING A FILE SYSTEM
Practices that use paper records may file records according to different methods. One method is to file alphabetically. All records are filed by the owner’s last name, then the first name. Other practices may file by client number. All pets are kept in the same file because many owners have more than one pet. Also included is a client/patient form (see Figure 2-8, A; Client Patient Information Sheet). Consent forms, patient check-in sheets, discharge sheets, and any other forms must be kept in this file as well.
PAPER RECORDS
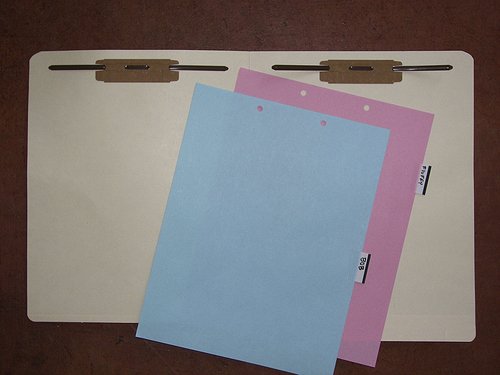
Paper records can either be classified as full paper records or index card records. Paper records are written on 8.5 × 11-inch paper and usually fastened into a file folder with a two-hole fastener (Figure 14-3).
 PRACTICE POINT
PRACTICE POINTEither file folders or index card holders can be alphabetized by client name or filed by client number, and colored letters and/or numbered labels can help identify those that are misfiled (Figure 14-4). Color coding the exterior of files can help identify misfiled charts from either the front or the back. Numbers indicating the year on the outside of the file can also help identify the last time a client has been into the practice, making it easier for team members to purge files efficiently. Alphabetical filing is the most common method used in practice. The last name, then first, along with a client identification number, are generally listed on the exterior of a file; the file is then alphabetized by the client’s last name.



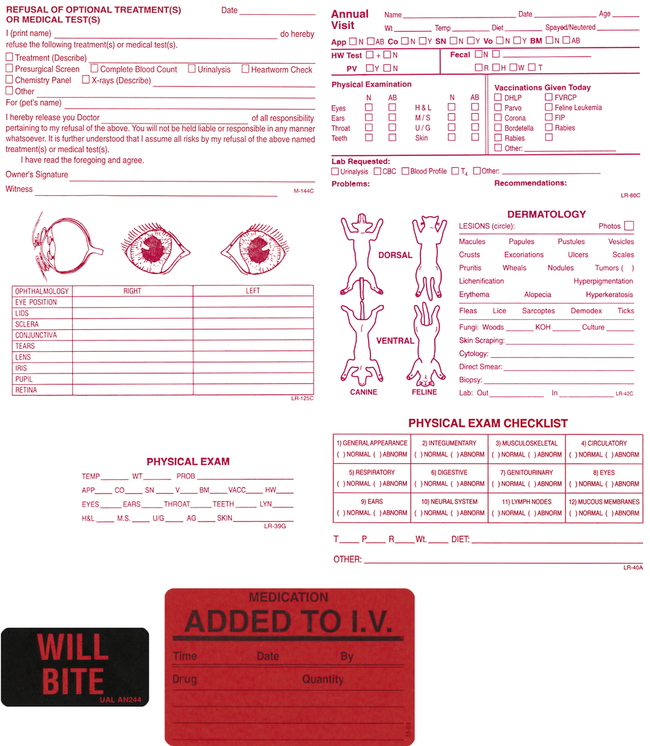
Colored warning stickers attached to patient medical records may draw attention to special medical needs. Sample stickers may include: “Will Bite!” “Anesthetic Alert!” or “Vaccine Reaction!” Figure 14-5 shows a variety if stickers that a practice may use in a paper record system. Bright-colored stickers can also be used on cage identification cards to alert team members of a patient’s special needs. A “Will Bite” sticker is beneficial for alerting team members to animals with which they must use special precautions.
 PRACTICE POINT
PRACTICE POINTCOMPUTERIZED MEDICAL RECORDS
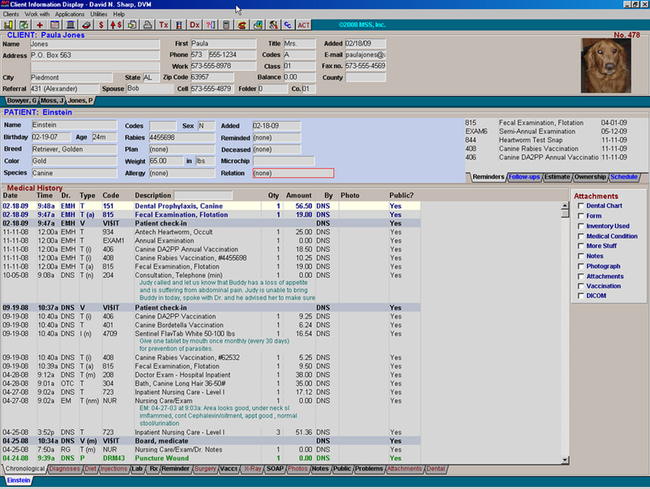
Computerized medical records, also referred to as paperless records, are filed in the computer by both client number and last name (Figure 14-6). Any record can be accessed from any computer. Lab work, radiographs, and ultrasound results are stored within the record. All charts, consent forms, and miscellaneous documents must be stored within the record. A practice that is truly paperless does not have any additional client files or folders that store release forms, lab work, or radiographs. Forms and lab work are scanned into the client’s record, or the client must sign the forms electronically, which are then stored in the computer. Radiographs are either in digital form or they are scanned into the record. Most lab work machines will enter results into the client’s file once the machine has completed the work. Client identification numbers must be verified before entering lab work to ensure the results will be populated into the correct records. When outside laboratory results are received, they can be electronically filed within the patient’s chart. An onscreen notice pops up for the veterinarian or staff when those results have become available.
 PRACTICE POINT
PRACTICE POINTPaper records and paperless records each have their advantages and disadvantages, all of which must be weighed when determining what is best for an individual practice (Box 14-2).
CHOOSING MEDICAL RECORD SOFTWARE
 PRACTICE POINT
PRACTICE POINTEfficiency of Computerized Laboratory Requisition Forms
Some laboratories work with veterinary practices to generate requisition forms online, creating a unique form and barcode. For example, IDEXX (Westbrook, Maine) LabREXX software (www.idexx.com/labrexx) works with existing veterinary practice software, allowing charges to be captured while ensuring no mistakes are made when submitting the client and patient name and doctor. To help increase efficiency, a quick guide of the most common tests the practice selects is available, allowing results to be emailed directly to clients and results to be downloaded to patient records. This prevents lost and/or misfiled results. Records are flagged, allowing the team to know that results have arrived in a patient’s file.
Chapter 8 gives a brief overview of software that is available in today’s market, along with a worksheet to help determine which software will work best for a veterinary practice.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


