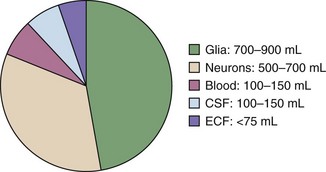
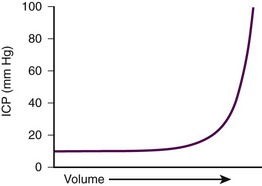
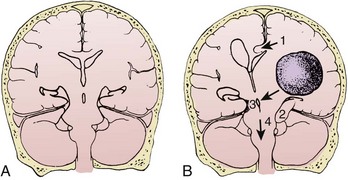
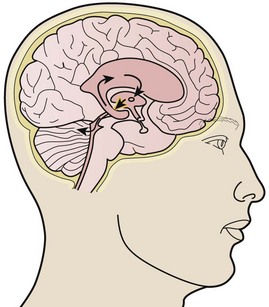
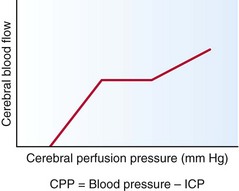
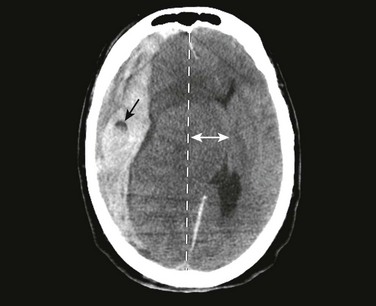
Chapter 59 The components of the calvaria are the brain parenchyma, cerebrospinal fluid (CSF), the venous blood supply, and the arterial blood supply (Fig. 59-1). CSF and the venous blood supply have the greatest ability to change their volume to compensate for increases in pressure. These dynamic changes in the relative proportion of the cranial content may not affect the patient if ICP is not excessive. However, if a pathologic process overwhelms the compensatory mechanisms, the result will be a nearly exponentially increase in ICP (Fig. 59-2). Normal supine ICP ranges from 5 to 15 mm Hg. Transient increases in ICP as high as 80 to 100 mm Hg occur with coughing or straining. Other factors that can transiently increase ICP are movement, pain, and fever. A space-occupying lesion such as a tumor, hematoma, abscess, or foreign body can also raise ICP. Figure 59-3 demonstrates that the area and cause of the increased ICP will determine where shifts occur to result in brain herniation. IIH, formerly known as pseudotumor cerebri, is a chronic condition characterized by increased CSF pressure not caused by a tumor, edema, hydrocephalus, or change in CSF composition. It occurs most frequently in obese women. Symptoms may include headache, nausea, and blurry vision. The headache is typically worse on waking or with exertion. In general, patients with IIH have normal findings on neurologic examination except for the frequent presence of papilledema. Although the precise pathophysiology remains unclear, severe cases can lead to permanent loss of vision. Commonly associated conditions are listed in Box 59-1. IIH is a diagnosis of exclusion. Because of its often subtle symptoms and normal findings on computed tomography (CT), it is often not suspected or diagnosed on initial clinical evaluation. Bleeding in the brain can occur spontaneously (as in the case of hemorrhagic stroke or spontaneous subarachnoid hemorrhage) or can be a result of trauma. In addition to the mass effect of the blood itself, the associated edema in both instances contributes to further increases in ICP. Diffuse axonal injury (DAI) may occur in isolation or in conjunction with intracerebral bleeding. With DAI it is believed that the axons are not actually torn, but instead suffer significant injury that may lead to edema (shearing effect).1 CSF is produced by the choroid plexus at a daily rate of 500 mL. It flows from the ventricles into the cisternae of the subarachnoid space and is drained by the arachnoid villi of the dural sinuses to maintain a constant volume of 100 to 150 mL. Obstructive hydrocephalus occurs when flow is blocked at any point in the ventricular system by clotted blood, tumor, colloid cyst, edema, or primary stenosis. Communicating hydrocephalus is due to impedance of flow beyond the ventricular system at the level of the basal cisternae or lack of absorption by the arachnoid villi. Communicating hydrocephalus can occur with both infection and subarachnoid hemorrhage (Fig. 59-4). Up to a certain range, cerebral blood flow (CBF) is maintained by an autoregulatory mechanism despite fluctuations in cerebral perfusion pressure (CPP) (Fig. 59-5). Constant CBF can typically be maintained at any CPP between 60 and 160 mm Hg. Once CPP is out of the autoregulatory zone, CBF is linearly related to CPP. CPP lower than 60 mm Hg can lead to ischemia, whereas CPP higher 160 mm Hg can result in hypertensive encephalopathy. Signs and symptoms of severely increased ICP include a decreasing level of consciousness, papilledema, cranial nerve palsies, and lateralizing neurologic deficits. When any of these are noted, particularly when CT confirms the presence of a mass effect such as hydrocephalus or a midline shift, urgent intervention is necessary (Fig. 59-6). Neurosurgical consultation for possible invasive means of reducing ICP and monitoring is indicated. Medical management of increased ICP should also proceed without delay. Rapid assessment of findings on the patient’s neurologic examination should be performed before sedation and paralysis (RSI). If time allows, premedicate the patient with lidocaine, 1 to 1.5 mg/kg, 3 minutes before intubation while preoxygenating the patient. Lidocaine has been reported to blunt the rise in ICP associated with laryngoscopy and may protect against some hypoxia-related dysrhythmias; however, its true value is unproven (see Chapters 4 and 5). Fentanyl is an excellent drug for control of pain, which if untreated, can lead to increased ICP. Fentanyl can also be given during the pretreatment phase of RSI (3 minutes before administration of the paralytic agent) if time allows. Caution should be exercised, however, to avoid precipitous drops in blood pressure, which can actually threaten CBF and exacerbate the brain injury. It is for this reason that we recommend titrating fentanyl up to the target dose rather than giving a full dose (typically 3 µg/kg) up front. We also recommend caution in brain-injured patients with concomitant trauma, who may have exaggerated episodes of hypotension with narcotics and sedatives. A defasciculating dose Induction (sedation) may be achieved with drugs that block the rise in ICP, such as etomidate (0.3 mg/kg intravenously [IV]), thiopental (50 to 100 mg IV or 3 to 5 mg/kg IV), or propofol (1 mg/kg IV).3–5 Etomidate is preferred over thiopental in patients with unstable hemodynamic status. Etomidate has two significant benefits—it has minimal effect on systemic blood pressure and does not appear to increase ICP.3,4 Propofol has gained acceptance as a sedative in patients with increased ICP because of its short duration of action and depression of cerebral metabolism and oxygen consumption. This may have a neuroprotective effect. However, propofol can cause profound decreases in systemic blood pressure and with higher doses and extended periods of use can be associated with significant morbidity.5 The paralytic agent of choice is succinylcholine (1.5 mg/kg in adults and up to 2.5 mg/kg in pediatric patients). Nondepolarizing agents are appropriate when contraindications to succinylcholine exist (see Chapter 5). Sedatives and paralytics should be short acting to facilitate close monitoring of the patient’s neurologic status. As the airway is secured, adequate supplemental oxygen should be provided, with titration down rapidly from the initial Fio2 of 1.0 used for RSI to ensure oxygen saturation greater than 90%.1 In general, avoid hyperventilation in patients with brain injury because low Pco2 levels cause cerebral vasoconstriction, which results in decreased CBF in the critical hours following injury.1,6 Hyperventilation is also associated with poor survival and neurologic outcomes.6,7 For the majority of brain-injured patients, the target is thus eucapnia with a Pco2 of 35 to 40 mm Hg.6 Nevertheless, if a patient displays evolving signs of brain herniation (e.g., anisocoria, hemiparesis, asymmetric posturing, Cushing’s reflex, or rapid deterioration in GCS score), hyperventilation may be necessary to arrest the process. Current recommendations target a Pco2 of 28 to 35 mm Hg in these scenarios as a temporizing measure until surgical intervention to lower ICP can occur.6 If not in shock, elevate the patient’s head to decrease ICP. This position allows drainage of cerebral veins. Feldman,8 Ng,9 and their colleagues demonstrated that elevation of the head to 30 degrees significantly reduces ICP in most patients without impairing CBF, CPP, or cerebral metabolism. Raising the head of a patient with hypotension, however, exacerbates any decrease in the patient’s mean arterial pressure (MAP) and hence lowers CPP. If head elevation is to be used, MAP must be maintained above 90 mm Hg to facilitate a CPP of approximately 60 mm Hg.10 It is also important to avoid neck rotation and flexion or any other intervention that could result in compression of the jugular vein. If the jugular veins are compressed, venous outflow from the head can be further compromised. The goal in fluid management is to maintain euvolemia; head-injured patients with hypotension have double the mortality of normotensive patients. Patients with increased ICP may be hypovolemic from profuse vomiting, decreased fluid intake, or hemorrhage. Distributive shock may also be present and occurs as a result of loss of vasomotor sympathetic tone, especially in patients with concomitant cervical spine injury. Only isotonic or hypertonic fluids should be used (normal or hypertonic saline) to avoid worsening the brain edema. Vasopressors may also be necessary. A target CPP of 60 mm Hg and MAP of greater than 90 mm Hg are recommended.11 Mannitol has two properties—it initially acts as a volume expander and then serves as an osmotic agent. On administration of mannitol, intravascular volume expands and blood viscosity decreases, which results in augmentation of CBF. Once volume expansion has occurred, osmotic movement of fluid from the cellular compartment to the intravascular compartment begins and results in a decrease in ICP. The osmotic effect usually occurs within 15 minutes. The half-life of mannitol ranges from 90 minutes to 6 hours.11 Its effect is most pronounced in patients with CPP lower than 70 mm Hg.11 Hypertonic saline is an alternative to mannitol in patients who are hypotensive. Theoretically, hypertonic saline is an ideal resuscitation fluid for patients with concomitant head injury and hemorrhagic shock because it can effectively expand intravascular volume while causing osmotic diuresis of the brain. However, its efficacy in human studies remains uncertain, so its use should be reserved for patients with contraindications to mannitol. Although hypertonic saline is generally administered in boluses of 100 to 250 mL of 3% to 7% saline, there is no consensus on the preferred concentration and volume of administration.11,12
Management of Increased Intracranial Pressure and Intracranial Shunts
Pathophysiology of ICP
Brain
CSF
Blood
Signs and Symptoms
Medical Treatment of Increased ICP
Sedation and Paralytics
 of the intubating dose of a nondepolarizing neuromuscular blocking agent may also be administered as pretreatment. If given 3 minutes before a paralyzing dose of succinylcholine, it counteracts the transient fasciculations and increase in ICP that occur with the administration of succinylcholine. It is important to note, however, that practice variations are common, and though theoretically attractive, none of these pretreatment options have been demonstrated to improve patient-oriented outcomes.2
of the intubating dose of a nondepolarizing neuromuscular blocking agent may also be administered as pretreatment. If given 3 minutes before a paralyzing dose of succinylcholine, it counteracts the transient fasciculations and increase in ICP that occur with the administration of succinylcholine. It is important to note, however, that practice variations are common, and though theoretically attractive, none of these pretreatment options have been demonstrated to improve patient-oriented outcomes.2
Oxygenation and Hyperventilation
Head Position
Fluid Management
Diuresis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Veterian Key
Fastest Veterinary Medicine Insight Engine