CHAPTER 58Late Term Pregnancy Monitoring
The equine biophysical profile was developed to help the clinician recognize and more accurately characterize the intrauterine problems in late-gestation mares that affect fetal well-being.1,2 The information obtained is used to formulate a treatment plan designed to improve the outcome, thereby decreasing fetal morbidity and mortality.1,2 The human biophysical profile has been routinely used to identify fetal and intrauterine conditions that predispose to fetal compromise, distress, or death in utero.3,4 Five variables are included in the human biophysical profile: fetal breathing movements, gross body movements, fetal tone, reactive heart rate, and a 2-cm (minimum) pocket of amniotic fluid.3,4 Each variable receives a score of 2 if the minimal criteria are met and 0 if they are not. To calculate the biophysical profile these scores are summed, resulting in a total score between 0 and 10 for each fetus. The biophysical profile is a measure of the well-being of the fetus, in particular the likelihood of acute or chronic fetal hypoxemia and asphyxia.3,4 The biophysical profile score is highly correlated with perinatal mortality and morbidity in the human fetus.3,4 A low score indicates fetal distress and the need for immediate intervention, whereas a high score is compatible with fetal well-being.3,4 The biophysical profile is used in late-gestation pregnancies to help the obstetrician decide when to intervene (either by inducing parturition or performing a cesarean section) and has helped reduce the incidence of fetal death.
DEVELOPMENT OF THE EQUINE BIOPHYSICAL PROFILE
The equine biophysical profile was developed after examining a normal population of mares in late gestation and three populations of high-risk pregnant mares.1,2,5,6 The normal population of late-gestation mares included normal pregnant mares who had ultrasonography performed in late gestation, no illness on admission, uneventful pregnancies, and normal foals. The high-risk pregnancies included all late-gestation pregnant mares who had ultrasonography performed and had an illness on admission, an abnormal parturition, and/or an abnormal foal. All fetuses were greater than 298 days’ gestational age at the time of the last examination. Mares whose foal was delivered by cesarean section were excluded from these studies. Earlier work by Adams-Brendemuehl and Pipers7–10 described the technique of transabdominal ultrasonography of the pregnant mare, normal findings during gestation, and abnormalities detected in late gestation as well as earlier in gestation.
ULTRASONOGRAPHIC EXAMINATION
Patient Preparation
The mare’s ventral abdomen is clipped with No. 40 surgical clipper blades from the xiphoid to the pubis and laterally to the level of the flank fold. The skin is then washed thoroughly with warm water and surgical scrub to free the skin of all the surface debris. Ultrasound coupling gel is then applied to the clipped area, and the ultrasonographic examination is performed. If image quality is poor, the ventral abdomen should be examined for areas that are poorly clipped or where surface debris remains on the skin. Applying warmed coupling gel may also help improve image quality. To perform the transcutaneous examination, unsedated mares are scanned from the ventral abdomen using a 2.5-, 3.0-, or 3.5-MHz transducer and a depth setting of 26 to 30 cm and a 5.0-, 6.0-, or 7.5-MHz transducer and a depth setting of 12 to 20 cm, as has been previously described.1,2,5,8–10 The lowest frequency transducer with the largest displayed depth available should be used for the initial uteral, fetal fluid, and fetal examination. The highest frequency transducer available that obtains a good-quality image with the smallest depth setting that displays the uterus and allantochorion should be used for the uteroplacental evaluations. The transcutaneous evaluation of the uterus, fetal membranes, and fetus are also combined with a transrectal fetal evaluation evaluating the uterus, the fetal membranes, fetal parts, and fetal fluids imageable from the transrectal window.
Fetal Assessments
Fetal Numbers
Fetal numbers are assessed. The typical “cut-pie” appearance of the nonfetal horn should be visible.
Fetal Position
Fetal position within the uterus is determined relative to the long axis of the mare.
Fetal Aortic Diameter
Fetal aortic diameter is measured from the leading edge to leading edge in the ascending aorta, close to the heart. Fetal aortic diameter is a reliable indicator of fetal size.1,2,5,6
Fetal Thoracic Diameter
Maximal fetal thoracic diameter is measured across the widest portion of the thorax at the level of the diaphragm (withers to girth if possible). This is a fairly good indicator of fetal size but less reliable than fetal aortic diameter.1,2,5,6
Fetal Breathing
The fetus is evaluated for the presence of breathing movements and their regularity. The excursions of the fetal ribs are assessed, and the diaphragm is evaluated for contractions. Fetal breathing should be evaluated for a minimum of 30 seconds in the absence of fetal movement.2,6
Fetal Cardiac Activity
Fetal heart rates and rhythm are obtained with M-mode echocardiography at rest and after fetal movement.1,2,6 The M-mode cursor is passed through any portion of the fetal heart where cardiac motion is detected, and an instantaneous fetal heart rate is obtained. Fetal heart rate can be obtained with instantaneous M-mode echocardiography in moving fetuses in most instances and is an indication of the normal heart rate variability in response to fetal movement.
Fetal Tone
Fetal tone is assessed as present or absent. Fetal tone is absent if the fetus appears limp.1,2,5,6
Maternal Assessments
Uteroplacental Thickness
The thickness of the uteroplacental unit is measured in each of the six areas (cranial, mid, and caudal on each side of the fetus). Measurements should be made in areas where the fetus is not lying against the ventral portion of the uterus, compressing the membranes.1,2,5,6 Both the maximal and minimal uteroplacental thickness should be obtained.6 Measurements should not be made in the nonfetal horn.1,2,5,6
NORMAL FINDINGS
Fetal Numbers and Presentation
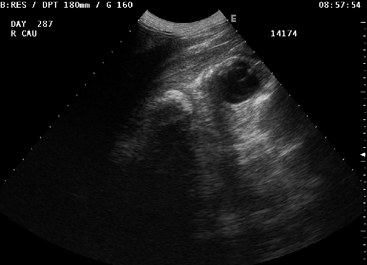
Normal mares in late gestation should have a single active fetus in anterior presentation.1,2 The fetal head should be visible from a transrectal window in late gestation but not from a transcutaneous window.2,6 Earlier in gestation until approximately 9 months, the fetus may be in any position. The fetal head may normally be imaged from the transcutaneous window before 298 days of gestation (Figure 58-1).
Fetal Aortic and Thoracic Diameter
The diameter of the fetal aorta (mean = 22.8 ± 2.15 mm) is significantly correlated with neonatal foal weight (P < 0.0008, r = 0.72) and maternal prepartum weight (P < 0.002, r = 0.86) in the late gestation fetus.1,2 The fetal aorta is recognized as the circular artery centrally located in the heart (Figure 58-2). Fetal aortic diameter and thoracic diameter increase gradually throughout gestation. There is a trend for the maximal thoracic diameter to be associated with neonatal foal weight. In the normal fetus the thoracic diameter is approximately 10 times the fetal aortic diameter. This relationship holds true throughout most of gestation.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


