Katherine S. Garrett
Laryngeal Ultrasound
Although upper airway endoscopy (both resting and dynamic) remains the mainstay for diagnosis of laryngeal and pharyngeal disorders, laryngeal ultrasonography can provide useful complementary information. Ultrasonography permits imaging of the laryngeal cartilages, the intrinsic laryngeal musculature, and portions of the hyoid apparatus. This allows a more thorough evaluation than is possible using endoscopy alone, which has implications for both diagnosis and treatment of conditions of the upper airway.
Equipment and Preparation
Examination of the larynx is performed with a linear or curvilinear ultrasound transducer operating at 8 to 10 MHz. A rectal probe can be used but is often less easy to manipulate for the operator. Generally, clipping of the haircoat is not required unless the hair is coarse or thick, although superior image quality can be obtained if the hair is clipped. The laryngeal region is saturated with isopropyl alcohol. An assistant or a stand should be used to support the horse’s head in an extended position, permitting access to the laryngeal region caudal to the mandible. Sedation with xylazine (0.4 mg/kg, IV) improves patient compliance and tolerance of the procedure.
Ultrasonographic Technique
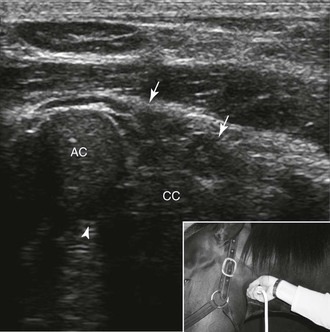
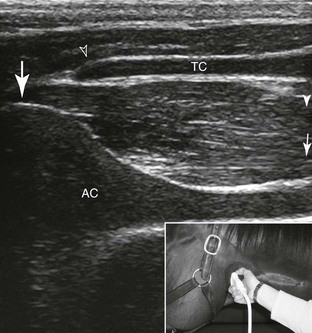
Images of the larynx are obtained in the dorsal and transverse planes from the lateral, dorsolateral, and ventral aspects. Positioning the transducer in the dorsal plane (horizontally) on the lateral aspect of the larynx (lateral window) allows imaging of the thyroid, cricoid, and arytenoid cartilages and the cricoarytenoideus lateralis and vocalis muscles (Figure 53-1). The transducer is moved dorsally and angled slightly ventrally to the dorsal oblique plane to image the lateral portion of the cricoarytenoideus dorsalis muscle from the dorsolateral aspect of the larynx (dorsolateral window; Figure 53-2) and the cricothyroid articulation. A longitudinal image of the thyroid and arytenoid cartilages and cricoarytenoideus lateralis and vocalis muscles is obtained from the lateral window by rotating the transducer to a vertical position, corresponding to the transverse plane of the larynx (Figure 53-3). The ventral aspect of the cricoid and thyroid cartilages, the vocal folds, and the basihyoid bone are imaged in the longitudinal and transverse planes from the ventral aspect of the larynx. Additional descriptions of ultrasonographic technique are available in the literature.

Pathologic Conditions
Recurrent Laryngeal Neuropathy
Horses with recurrent laryngeal neuropathy undergo neurogenic atrophy of the adductor and abductor muscles of the arytenoid cartilage that are innervated by the recurrent laryngeal nerve. Endoscopically, this is manifested as incomplete or absent arytenoid cartilage abduction. Clinical signs associated with incomplete arytenoid cartilage abduction include abnormal upper airway noise, exercise intolerance, and poor performance.
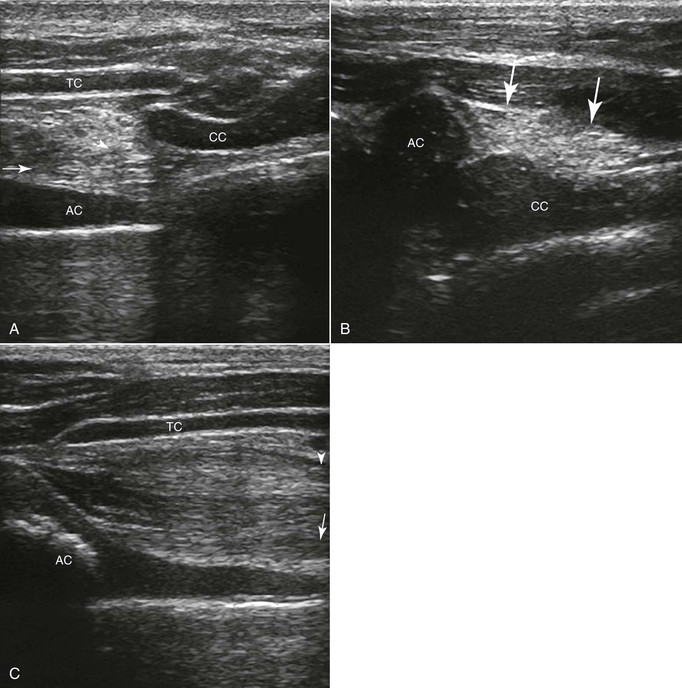
Horses with recurrent laryngeal neuropathy have characteristic ultrasonographic findings, specifically an increase in echogenicity of the cricoarytenoideus lateralis, cricoarytenoideus dorsalis, and vocalis muscles, compared with the contralateral side (Figure 53-4). This increase in echogenicity is thought to be a result of replacement of the normal muscular tissue with fibrous tissue and fat, a consequence of denervation atrophy. Because the increase in echogenicity of the musculature is determined subjectively through comparison to the opposite side or to muscles not innervated by the recurrent laryngeal nerve (e.g., the cricothyroideus muscle), experience with the technique improves accuracy.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


