Chapter 119Lameness in the Polo Pony
Polo as an Industry
Today three types of polo are played: outdoor, indoor (arena), and snow polo. Outdoor polo is by far the most popular and is played on a large, finely manicured grass field measuring 274 m (300 yards) by 137 m (150 yards) (Figure 119-1). Injuries are related to fatigue (because of the distances covered), stopping, turning, speed, and surface consistency, depending whether the soil beneath the grass is compact or soft. Arena polo is played in much smaller arenas and is more common in collegiate settings. Injuries tend to be less frequent and are usually impact related. Snow polo is regarded as a novel exhibition sport played on the surface of a frozen lake and produces surprisingly few injuries. Obviously, footing and surface conditions often can be responsible for the type of lameness seen. Heavy, soft, grass polo fields and deep, sandy, uneven exercise tracks are frequently responsible for proximal suspensory desmitis (PSD), suspensory branch desmitis, and metacarpophalangeal joint sprains. Hard fields, exercise tracks, and polo field sideboards may cause hoof and pastern region injuries, and hard, fast ground predisposes horses to superficial digital flexor (SDF) tendonitis.

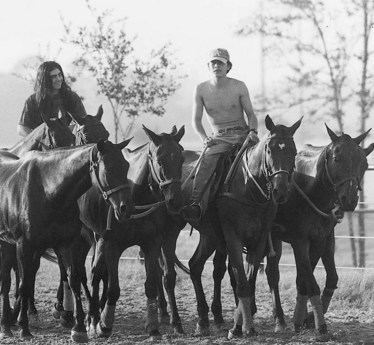
Neck reining is paramount in training a polo prospect because the rider uses only one hand for control. Wide range of movement, the ability to stop and turn quickly, and the ability to exhibit rapid bursts of speed are required. How well and smoothly the horse performs these maneuvers often determines the number of years the horse stays sound and competes successfully. In addition to schooling, fitness training consists of daily galloping (legging up). Ponies often are tied together in sets of four to five. This time-saving practice teaches the horses to travel more calmly together in close contact but can result in traumatic injuries to the lower limbs (Figure 119-2).
Lameness Examination
Hindlimb PSD has become a common diagnosis because we are now more aware of it. In the United Kingdom, a variation of the high plantar nerve block, analgesia of the deep branch of the lateral plantar nerve (see Chapter 10), is commonly used to diagnose PSD. Three milliliters of local anesthetic solution is injected deep to the proximal aspect of the lateral splint bone, and 2 mL each is placed over the medial and lateral plantar nerves. If this block is unsuccessful in abolishing pain, each hock joint compartment is blocked subsequently. This procedure then is followed by fibular and tibial nerve blocks. In Argentina, chemical neurolysis (long-term nerve block) of the fibular and tibial nerves frequently is performed for horses with distal hock joint pain or PSD (PJM).
Ten Most Common Lameness Problems in Polo Ponies
Superficial Digital Flexor Tendonitis
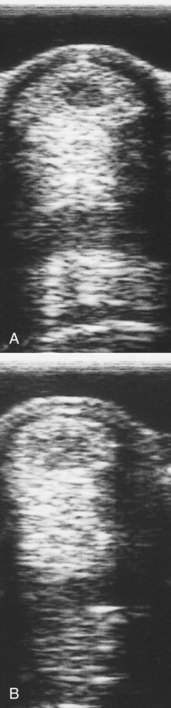
We believe that most peripheral injuries of the SDFT result from tendon trauma while the limb is bearing weight. However, the Editors note that peripheral injuries commonly are seen in other sports horses, such as Standardbred racehorses and reining horses, in which direct trauma is usually not a factor. These injuries occur much more frequently at the midmetacarpal region on the lateral aspect and to a lesser extent on the palmar surface of the tendon (Figure 119-3). Proximal SDF tendonitis also can be caused by trauma (PJM). These areas have a high degree of exposure to swinging mallets and flying hooves. Despite new protective boots, the SDFT is still traumatized with surprising frequency. Traumatic tendon injuries are generally noticed 1 to 2 days after the incident and are characterized by a slight widening of the tendon (not a banana-shaped profile). Lameness is usually not present, but the area is warm and tender to palpation. Some horses have recurrent heat and swelling that resolves quickly with topical and systemic antiinflammatory therapy. Peripheral tendon fiber lesions may involve 20% or less of the cross-sectional area (CSA) of the tendon. However, careful ultrasonographic examination of the medial and lateral borders of the SDFT and critical evaluation of longitudinal images are necessary. Recurrent tendonitis leads to typical swelling and later lameness commonly found with moderate or severe SDF tendonitis.
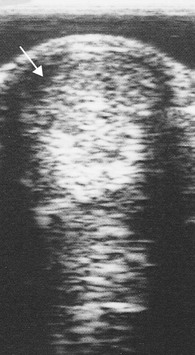
Core lesions and lesions of the SDFT adjacent to the DDFT are thought to be injuries related to speed and fatigue. Hard, fast ground may be a predisposing factor. SDF tendonitis may result in a banana-shaped profile of the metacarpal region. Core lesions compromising between 20% and 25% of the CSA of the SDFT are serious, and the risk of recurrence is high (Figure 119-4). Horses with small CSA tears that extend more than 2.5 cm in length or those with distally located tendonitis involving SDFT impingement by the palmar annular ligament (PAL) are at high risk of recurrence. Despite appropriate therapy, these horses often have chronic and recurrent lameness, and ultrasonographic evaluation reveals a lesion that often fails to heal.