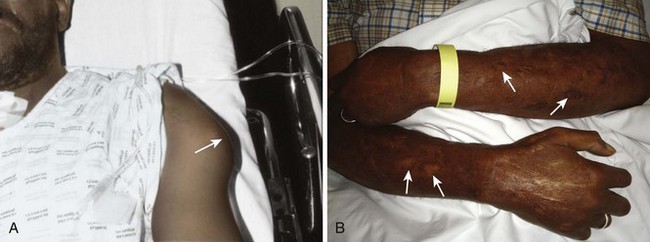
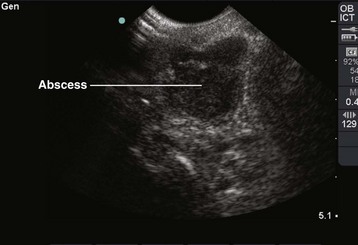
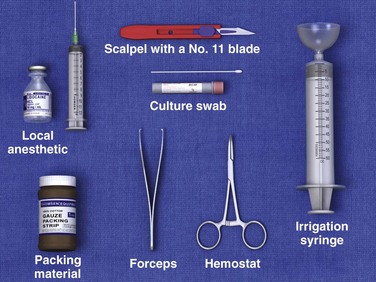
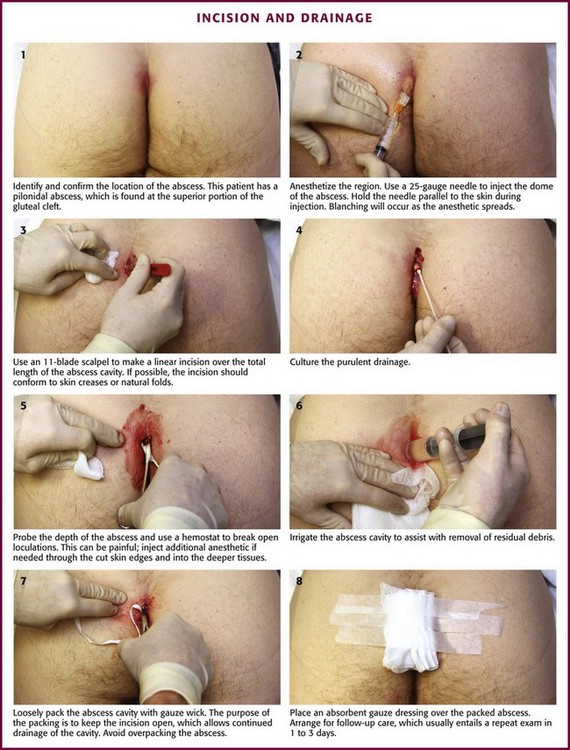
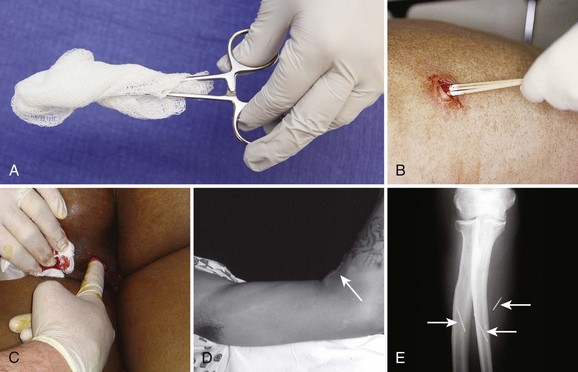
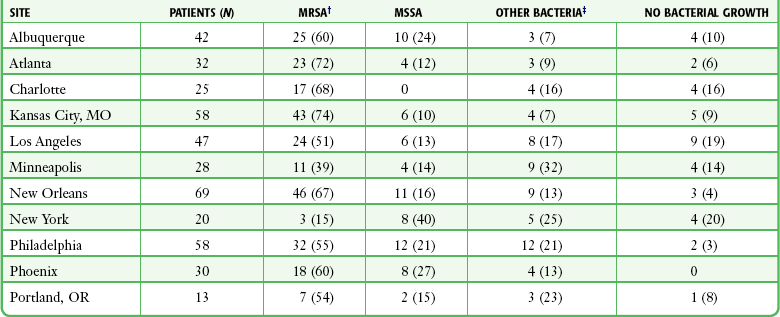
Chapter 37 Incision and drainage (I&D) procedures in the emergency department (ED) are most commonly performed for soft tissue abscesses (Fig. 37-1).1,2 The total number of ED visits increased from 90 million to 115 million over a 10-year period, with visits for abscess-related complaints increasing faster than overall ED visits.3 An abscess typically starts as a local superficial cellulitis. Various organisms that colonize normal skin can cause necrosis and liquefaction with subsequent accumulation of leukocytes and cellular debris. Loculation and subsequent walling off of these products lead to abscess formation. The cause of localized abscesses depends on the anatomic location, and they are usually caused by the flora indigenous to that area. Different organisms cause disease based on environmental exposure. For example, direct inoculation of extraneous organisms may occur during a mammalian bite (e.g., Eikenella, Pasteurella), exposure to saltwater (e.g., various Vibrio strains) or freshwater (e.g., Aeromonas), or meat or fish exposure (e.g., Erysipelothrix rhusiopathiae). Pseudomonas folliculitis has been associated with the use of whirlpools.4 Staphylococcal strains, which are normally found on the skin, produce rapid necrosis, early suppuration, and localized infections with large amounts of creamy yellow pus—the typical manifestation of an abscess. Conversely, group A β-hemolytic streptococcal infections tend to spread through tissues and cause a more generalized infection characterized by erythema, edema, a serous exudate, and little or no necrosis—typical manifestations of cellulitis. Anaerobic bacteria, which proliferate in the oral and perineal regions, produce necrosis with profuse brownish, malodorous pus5 and may cause both abscesses and cellulitis. Normal skin is extremely resistant to bacterial invasion, and few organisms are capable of penetrating intact epidermis. In a normal healthy host with intact skin, the topical application of even very high concentrations of pathogenic bacteria does not result in infection. The requirements for infection usually include a high concentration of pathogenic organisms, such as in hair follicles in the adnexa; occlusion of glands or other structures that prevent desquamation and normal drainage; a moist environment; adequate nutrients; and trauma to the corneal layer, which allows organisms to penetrate into deeper tissues.6 Tissue perfusion may also play a role in the ability to prevent infection. Trauma may be the result of abrasions, shaving, insect bites, hematoma, injection of chemical irritants, incision, or occlusive dressings that macerate the skin. The presence of a foreign body can potentiate skin infections by enabling a lower number of bacteria to establish an infection. For example, abscesses occasionally develop at suture sites in otherwise clean wounds. In addition, abscesses can develop at any site used for body piercing. “High” ear piercings (through the cartilage of the pinna) seem to be at particular risk for infection because of the avascularity of auricular cartilage.7 When favorable factors are present, the normal flora that colonize cutaneous areas flourish and infect the skin and deeper structures. In persons performing manual labor, the arms and the hands are infected most frequently. In women, the axilla and submammary regions are frequently infected because of minor trauma from shaving, contact with garments, a moist environment, and an abundance of bacteria in these areas. Infections may develop anywhere on the body in intravenous (IV) drug users, although the upper extremities are most commonly affected.8,9 Deep soft tissue abscesses can be caused by an addict’s attempts to access deep venous structures when peripheral venous access sites are exhausted.10 In addition, areas with compromised blood supply are more prone to infection because normal host defenses, including cell-mediated immunity, are less available.7 Although most abscesses contain bacteria, 5% of abscesses are sterile, especially those associated with IV drug use. Clinically, sterile abscesses cannot be differentiated from those caused by bacteria. Somewhat atypical abscesses develop in parenteral drug users. Injection of a cocaine-heroin mixture (“speedball”) may predispose users to abscesses by inducing soft tissue ischemia.11 Bergstein and coworkers9 found anaerobes in 143 of 243 isolates from 57 drug-abusing patients. Abscesses at the site of injection tend to contain predominantly staphylococcal and streptococcal species. However, some drug users lubricate their hypodermic needles with saliva, which potentially explains the isolation of oral pathogens such as Eikenella corrodens from injection site abscesses. In 2002, Brook12 compiled the findings from more than 15 bacteriologic studies of 676 polymicrobial abscesses. S. aureus and group A β-hemolytic streptococci were the most prevalent aerobes in skin and soft tissue abscesses and were isolated in specimens from all body sites. Gastrointestinal and cervical flora (enteric gram-negative bacilli and Bacteroides fragilis) were found most often in intraabdominal, buttock, and leg lesions. Group A β-hemolytic streptococci, pigmented Prevotella, Porphyromonas species, and Fusobacterium species—all normal residents of the oral cavity—were most commonly found in lesions of the mouth, head, neck, and fingers. In a study of the bacteriology of cutaneous abscesses in children, Brook and Finegold13 found aerobes (staphylococci and group A β-hemolytic streptococci) to be the most common isolates from abscesses of the head, neck, extremities, and trunk, with anaerobes predominating in abscesses of the buttocks and perirectal sites. Mixed aerobic and anaerobic flora was found in the perirectal area, head, fingers, and nail bed. This study noted an unexpectedly high incidence of anaerobes in nonperineal abscesses. Anaerobes were found primarily in areas adjacent to mucosal membranes (e.g., the mouth), where these organisms tend to thrive, and in areas that are easily contaminated (e.g., by sucking fingers, which causes nail bed and finger infections or bite injuries). If an unexpected or atypical organism is found in an abscess culture, the clinician should consider an underlying process not readily apparent from the history or physical examination. For example, tuberculosis or fungal isolates are sometimes found in immunocompromised patients (e.g., those with diabetes or acquired immunodeficiency syndrome). Finding Escherichia coli suggests an enteric fistula or even self-inoculation of feces in some patients with a psychiatric illness such as Munchausen’s syndrome. Recurrent abscesses without an obvious underlying cause could indicate clandestine drug use. What appears to be a typical recurrent abscess may be a manifestation of an underlying septic joint, osteomyelitis, or rarely, metastatic or primary cancer (Fig. 37-2). Parenteral drug users, insulin-dependent diabetics, hemodialysis patients, cancer patients, transplant recipients, and individuals with acute leukemia have an increased frequency of abscess formation when compared with the general population. At initial evaluation the patient may emphasize an exacerbation of the underlying disease process or an unexplained fever, with symptoms of an abscess being a secondary complaint. In this situation, abscesses tend to have exotic or uncommon bacteriologic or fungal causes and typically respond poorly to therapy.14–17 Patients with diabetes-induced ketoacidosis (DKA) should be evaluated extensively for an infectious process; a rectal examination should be included with the physical examination to rule out a perirectal abscess as the infectious trigger of DKA. This is also true for patients who are immunocompromised. There are several reasons why patients with diabetes and parenteral drug users are at increased risk for abscess formation: intrinsic immune deficiency, an increased incidence of staphylococcal carriage, potentially compromised tissue perfusion, and frequent needle punctures, which allow a mode of entry for pathogenic bacteria.18 Drug users frequently use veins in the neck and in the femoral areas, which can produce abscesses and other infectious complications at these sites.19 Any abscess near a vein of the antecubital fossa or dorsum of the hand should alert the clinician to possible IV drug use; however, substance users may also inject directly into the skin (“skin popping”), which can cause cutaneous abscesses distant from veins (Fig. 37-3). A foreign body may serve as a nidus for abscess formation. IV drug users frequently break needles off in skin that has been toughened by multiple injections, so the clinician should maintain a high index of suspicion for retained needle fragments. If an abscess is recurrent or if the patient is a known or suspected IV drug user, consider radiographs or other techniques to search for foreign bodies, an underlying septic joint, or osteomyelitis.20 Ultrasound is also a useful adjunct to evaluate for foreign bodies that are not radiopaque. First acknowledged in the 1960s as a cause of infection in patients in health care settings, MRSA has now become the most common identifiable cause of community-acquired skin and soft tissue infections in many metropolitan areas in the United States. The spread of this organism is considered an epidemic, and it is a very virulent and aggressive.21,22 Virulent community-acquired MRSA (CA-MRSA) causes rapid and destructive soft tissue infection because of the presence of two bacterial toxins elaborated by the omnipresent VSA-300 and VSA-400 strains. Panton-Valentine leukocidin enhances tissue necrosis, and phenol-soluble modulin is toxic to neutrophils. A small pustule can become a large abscess in 24 to 48 hours (Fig. 37-4). Such lesions are often mistaken for a spider bite or drug use because of their rapid progression and seemingly spontaneous onset in an otherwise healthy person. Methicillin resistance is mediated by PBP-2a, a penicillin-binding protein encoded by the mecA gene that permits the organism to grow and divide in the presence of methicillin and other β-lactam antibiotics. S. aureus acquires methicillin resistance through a mobile staphylococcal cassette chromosome (SCC) that contains the mecA gene complex (SCCmec). MRSA probably arose as a result of antibiotic selective pressure.23,24 A single clone probably accounted for most MRSA isolates discovered during the 1960s; by 2004, six major MRSA clones had emerged.25 The spread of resistance is thought to be mediated by horizontal transfer of the mecA gene and related regulatory sequences thereon.26 In 1980, the spread of MRSA from hospitals into communities became evident. More recently, community-acquired infections have occurred more frequently, even in people without known risk factors. These observations have led to the identification of some risk factors for CA-MRSA (Box 37-1), including skin trauma (e.g., lacerations, tattoos, IV and intradermal drug use, shaving), incarceration, shared razors or towels, and close contact with others colonized or infected with MRSA.27–35 Animals can also carry MRSA and can function as a source of transmission.36 Importantly, many patients with CA-MRSA have no identifiable risk factors for acquisition of the disease.37 CA-MRSA tends to be more virulent than health care–associated MRSA (HA-MRSA) and is associated with more frequent serious complications such as osteomyelitis, joint infections, sepsis, and death. However, these organisms fortunately tend to be susceptible to a broader array of antibiotics.38 The prevalence of MRSA has increased in both health care and community settings. For example, the prevalence of methicillin resistance among S. aureus isolates in intensive care units in the United States was 60%,21 and more than 90,000 invasive infections by MRSA occurred in the United States in 2005.39 HA-MRSA and CA-MRSA differ with respect to their clinical epidemiology and molecular structures. HA-MRSA is defined as MRSA infection that occurs following hospitalization (hospital onset, formerly “nosocomial”) or MRSA infection that occurs outside the hospital within 12 months of exposure to a health care setting (e.g., history of surgery, hospitalization, dialysis, or residence in a long-term care facility—community onset instead of community acquired).21 HA-MRSA is usually associated with severe, invasive disease, including skin and soft tissue infection, bloodstream infection, and pneumonia.6,40 In fact, S. aureus continues to be a significant cause of surgical site infections.39 HA-MRSA strains tend to be resistant to multiple drugs. MRSA is one of the few pathogens routinely implicated in nearly every type of hospital-acquired infection. This is probably related in part to the organism’s capacity for biofilm formation on indwelling lines and tubes in hospital settings.24 Biofilm facilitates survival and multiplication of MRSA on these surfaces, thereby prolonging the duration of exposure of the organism to antibiotics, as well as promoting the potential for the development of genetic resistance.27 CA-MRSA is defined as MRSA infection that occurs in the absence of health care exposure. It is often associated with skin and soft tissue infections in young, otherwise healthy individuals.27 Most CA-MRSA strains are sensitive to non–β-lactam antibiotics, although a multidrug-resistant isolate has been described in men who have sex with men.41,42 This strain contains the pUSA03 plasmid and carries resistance genes for β-lactams, fluoroquinolones, tetracycline, macrolides, clindamycin, and mupirocin. The CA-MRSA and HA-MRSA classifications are no longer distinct since MRSA colonization can develop in one realm and manifestations of infection in another. In the mid-2000s in San Francisco, the annual incidence of CA-MRSA surpassed that of HA-MRSA.43 Furthermore, community-onset HA-MRSA infections have been observed with increasing frequency. This was illustrated in a study of 209 patients discharged from hospitalized care; within 18 months following hospital discharge, 49% of new MRSA infections began outside the hospital.44 In another series of 102 patients with CA-MRSA infections, 29% had molecular typing consistent with HA-MRSA.45 CA-MRSA was initially reported in injection drug users in the early 1980s and has since become the most frequent cause of skin and soft tissue infections seen in U.S. EDs and ambulatory clinics. In an assessment of the prevalence of MRSA across the United States, Moran and colleagues46 compiled data from adults who sought treatment of acute skin and soft tissue infections in EDs in 11 American cities in August 2004. S. aureus was isolated from three fourths of the 422 patients who met the study criteria. Seventy-eight percent of the S. aureus isolates were resistant to methicillin. MRSA was isolated from 59% of patients in the study. The prevalence of MRSA ranged from 15% to 74% in the participating EDs (Table 37-1). MRSA was the most common identifiable cause of skin and soft tissue infections in all but one of the EDs. TABLE 37-1 Bacterial Isolates from Purulent Skin and Soft Tissue Infections in U.S. EDs* *Thirty-one cultures, including 10 from which MRSA was isolated, were polymicrobial. Because of rounding, percentages may not total 100. †P < 0.001 for the test for homogeneity of MRSA prevalence across sites. ‡Other bacterial isolates were as follows: MSSA (17%), Streptococcus species (7%), coagulase-negative staphylococci (3%), and Proteus mirabilis (1%). From Moran GJ, Krishnadasan A, Gorwitz RJ, et al, for the EMERGEncy ID Net Study Group. Methicillin-resistant S. aureus infections among patients in the emergency department. N Engl J Med. 2006;355:666-674. Frazee and associates,38 reporting from an ED in northern California, found that half of the 137 patients in their study were either infected with or colonized by MRSA. Three fourths of all S. aureus isolates were MRSA. In addition, 76% of cases met a strict clinical definition of CA-MRSA. The incidence of CA-MRSA, genetically unrelated to nosocomial isolates, increased steadily from 1990 to 2001 and then dramatically in 2002 and each year thereafter.47,48 MRSA has also emerged as a potential sexually transmitted disease. Roberts and colleagues described their treatment of two patients who came to their urban ED with abscesses probably transmitted by heterosexual oral-genital contact. Both tested positive for MRSA.22 A 2010 case report drew a similar conclusion. It reported orogenital transmission of MRSA to an immunocompetent 22-year-old man who tested orally positive for MRSA and group B (genital) Streptococcus after oral contact with a female partner in whom MRSA-positive gluteal lesions had previously been diagnosed.48 In a retrospective chart review, Roberts and colleagues found that 18% of the 524 subcutaneous abscesses treated in their urban ED in 2006 were confined to the genital area. Almost three fourths of the 272 outpatient wound cultures performed on that year’s patient population were positive for MRSA.22 The diagnosis of cutaneous abscess formation is usually straightforward. The presence of a fluctuant mass in an area of induration, erythema, and tenderness is clinical evidence that an abscess exists (see Fig. 37-1). An abscess may appear initially as a definite tender soft tissue mass, but in some cases, a distinct abscess may not be readily evident. If the abscess is deep, as is true of many perirectal, pilonidal, and breast abscesses, the clinician may be misled by the presence of a firm, tender, indurated area without a definite mass. If the findings on physical examination are equivocal, needle aspiration or ultrasound examination may be performed to assist in the diagnosis.49 This approach may also identify a mycotic aneurysm or an inflamed lymph node simulating an abscess. A specific entity commonly mistaken for a discrete abscess is the sublingual cellulitis of Ludwig’s angina (see Chapter 64). Parenteral injection of illicit drugs can produce simple cutaneous abscesses that unpredictably advance to extensive necrotizing soft tissue infections. The emergency clinician must maintain a high index of suspicion to avoid missing this potentially life-threatening condition.8 Cellulitis and abscess formation can lead to bacteremia and sepsis, especially in immunocompromised patients. Cellulitis and Abscesses by Christine Butts, MD Ultrasound offers a distinct advantage when evaluating a patient with suspected soft tissue infection and may change management. A recent study from Academic Emergency Medicine by Tayal and colleagues evaluated the effect of soft tissue ultrasound on the management of cellulitis in the emergency department.1 The authors found that in patients with a low suspicion for abscess, ultrasound changed management in 56% of cases. Peritonsillar abscesses are difficult to diagnose from the physical examination alone, and some clinicians may feel hesitant to attempt blind drainage. Ultrasound of suspected peritonsillar abscesses has been found to be reliable in making the diagnosis. The overall size of the abscess, as well as its proximity to the carotid artery, can be evaluated with ultrasound, which will perhaps improve the confidence of the clinician in attempting drainage.2,3 Normal soft tissue is characterized by well-defined layers, with clear demarcation between these layers (Fig. 37-US1). The top of the screen corresponds to the most superficial soft tissue, including the epidermis and dermis. It should appear hyperechoic (light gray to white), thin, and clearly separate from the underlying layers. Subcutaneous tissue is found beneath the dermis and is of varying thickness. However, as with the most superficial layers, this layer should appear thin and well demarcated from the surrounding layers. Underneath the subcutaneous tissue, muscle will typically be seen as layers of striated tissue separated by bright layers of fascia. Cellulitis is recognized on ultrasound by thickening of the skin and subcutaneous layers (Fig. 37-US2). The tissue may also appear more hyperechoic than normal soft tissue. When a significant amount of edema is present within the tissue, bands of hypoechoic (dark gray) or anechoic (black) fluid may be seen within the area of thickened tissue. This is known as “cobblestoning” (Fig. 37-US3). Cobblestoning appears as thin bands of fluid throughout the tissue and can be distinguished from an abscess by the lack of a discrete fluid collection. An abscess is seen as a focal, discrete fluid collection within an area of cellulitis (Fig. 37-US4). The presence of surrounding cellulitis is the key to distinguishing an abscess from other fluid collections such as cysts. The character of the fluid may be variable, depending on the content of the abscess. Collections that are completely fluid will appear as anechoic (black) areas, whereas areas with more solid components will appear to have “internal echoes” within the collections (Fig. 37-US5). Once a focal fluid collection has been located, it can be evaluated in detail to determine the overall size and depth from the surface. Peritonsillar abscesses appear as rounded hypoechoic (dark gray) to anechoic (black) collections of variable size. In addition to confirming the presence of an abscess, the location and depth of the carotid artery can also be judged before an attempt at aspiration. 1. Tayal, VS, Hasan, N, Norton, HJ, et al. The effect of soft-tissue ultrasound on the management of cellulitis in the emergency department. Acad Emerg Med. 2006;13:384–388. 2. Blaivas, M, Theodoro, D, Duggal, S. Ultrasound-guided drainage of peritonsillar abscess by the emergency physician. Am J Emerg Med. 2003;21:155–158. 3. Lyon, M, Blaivas, M. Intraoral ultrasound in the diagnosis and treatment of suspected peritonsillar abscess in the emergency department. Acad Emerg Med. 2005;12:85–88. A complete blood count (CBC), blood cultures, and Gram stain are not standard or required for the treatment of straightforward cutaneous abscesses in the ED. Recommendations for culturing abscesses encountered in the ED are confusing, and clinical practice varies. Firm recommendations for the emergency clinician are difficult to standardize, partly because of insufficient data but also because the recommendations promulgated are not confined to ED abscess treatment. In addition, “complicated” and “uncomplicated” criteria are somewhat arbitrary. Traditionally, culturing the contents of a readily drainable cutaneous abscess was not indicated, nor standard. It simply provided no useful information to the clinician under most circumstances. Many clinicians still forgo routine culturing, even in the CA-MRSA milieu. Currently, there is no agreed on standard concerning routine culturing, and reasonable arguments can be made for a culture or no-culture approach to most abscesses treated in the ED. The authors support selective, not routine culturing but acknowledge that some now consider cultures to be indicated for all abscesses drained in the ED. A culture will potentially identify an unusual or resistant organism, especially if I&D is not curative. Culture will also permit identification of antibiotic susceptibility and assist in customization of antibiotic therapy. Cohort results also provide a framework for local epidemiology and resistance patterns. Culturing the abscess contents will distinguish between MRSA and nonresistant abscesses and will provide useful sensitivity information when managing complicated cases. Culturing should be performed for recurrent, unusual, or atypical abscesses. This information could be useful if the patient responds poorly to initial surgical drainage, if secondary spread of the infection occurs, or if bacteremia develops.50,51 It also appears prudent to obtain cultures from abscesses and other purulent skin and soft tissue infections in patients already taking antibiotics, in immunosuppressed patients, in those with signs of systemic illness, in patients who have not responded adequately to initial treatment, if there is concern for a cluster or outbreak of infection, or in patients with severe local infection.51 Severe local infection can be defined as an abscess larger than 5 cm in diameter, multiple lesions, or extensive surrounding cellulitis. However, the degree of surrounding cellulitis qualifying as “extensive” is ill defined. The discovery of solid or suspicious material in an abscess should prompt histologic evaluation since a malignancy may mimic cutaneous abscesses (see Fig. 37-2A and B). Gram stain is neither indicated nor standard in the care of uncomplicated simple abscesses. However, patients who appear “toxic” or immunocompromised and those who require prophylactic antibiotics (see the section “Prophylactic Antibiotics” later in this chapter) may benefit from Gram stain in addition to cultures. Gram stain results have been shown to correlate well with subsequent culture results, so in compromised hosts the test can be used to direct the choice of antibiotic therapy. Anaerobic infections should be suspected when multiple organisms are noted on Gram stain, when a foul odor is associated with the purulence, when free air is noted on radiographs of the soft tissue, and when no growth is reported on cultures.12 Surgical I&D is the definitive treatment of a soft tissue abscess52; antibiotics alone are often inadequate. Drainage of a suppurative focus generally results in marked resolution of the symptoms in most uncomplicated cases. In the initial stages, only induration and inflammation may be found in an area destined to produce an abscess. Premature incision, before localization of pus, will not be curative and may theoretically be deleterious because extension of the infectious process and, rarely, bacteremia can result from manipulation. In some cases, the application of heat to an area of inflammation may ease the pain, speed resolution of the cellulitis, and facilitate the localization and accumulation of pus. Nonsurgical methods are not a substitute for surgical drainage and should not be continued for more than 24 to 36 hours before the patient is reevaluated. The duration of therapy for skin and soft tissue infections has not been well defined, although no differences in outcome were observed in adult patients with uncomplicated cellulitis receiving 5 versus 10 days of therapy in a randomized, controlled trial.53 In the Food and Drug Administration licensing trials for complicated skin and soft tissue infections, patients were typically treated for 7 to 14 days. However, in the outpatient setting of uncomplicated infections, 3 to 5 days of antibiotic therapy is reasonable but should be individualized on the basis of the patient’s clinical condition and response to treatment. Accordingly, a return wound inspection or primary care follow-up is an important component of the care plan. IV drug users with an abscess and fever require parenteral antibiotic therapy after blood has been drawn for culture until bacterial endocarditis can be ruled out.50 Additionally, patients who have extensive cellulitis or are clinically septic require immediate IV antibiotics, as well as aggressive surgical drainage of pus. By administering IV ampicillin/sulbactam (2 g/1 g) every 6 hours, Talan and colleagues51 achieved 100% eradication of pathogens from major abscesses in hospitalized IV drug users and non–drug users. In contrast to prophylaxis before surgery, the routine use of therapeutic oral antibiotics after I&D of simple cutaneous abscesses in otherwise healthy patients who are not immunocompromised appears to have no value, and their empirical use cannot be scientifically supported. Llera and Levy52 performed a randomized, double-blind study to compare the outcomes of patients treated with a first-generation cephalosporin after the drainage of cutaneous abscesses in the ED with those who received placebo. They found no significant difference in clinical outcome between the two groups and concluded that antibiotics are unnecessary for abscesses in individuals with normal host defenses. This is in agreement with several previous studies.54–56 It should be noted that high-risk patients were often excluded from these studies. Immunocompromised patients have not been adequately studied in this situation and are therefore often given antibiotics empirically, but this practice, though common, has not been supported by rigorous prospective studies. The precise risk for endocarditis after I&D of a cutaneous abscess remains unknown, and it is difficult to predict in which patients an infection will develop and which particular therapeutic procedures subject the patient to the highest risk for infection. However, bacteremia clearly occurs with manipulation of infected tissue, and mortality rates are substantial for MRSA-associated endocarditis (30% to 37%).57,58 Given this risk, it is reasonable that patients at highest risk for cardiac complications related to transient bacteremia be pretreated with appropriate antibiotics within 1 hour preceding the procedure.59–61 Guidelines issued by the American Heart Association (AHA) in 2007 recommend antibiotic prophylaxis for procedures involving the respiratory tract or involving infected skin or musculoskeletal tissue only in patients with cardiac conditions that carry the highest risk for an adverse outcome from infective endocarditis.60 These conditions are listed in Box 37-2. Most skin infections are polymicrobial, but only staphylococci and β-hemolytic streptococci are likely to cause infective endocarditis. Therefore, the therapeutic regimen should include an agent active against these organisms, such as an antistaphylococcal penicillin or a cephalosporin. For patients who cannot tolerate a β-lactam or if MRSA is suspected, vancomycin or clindamycin can be substituted. Cutaneous abscesses may result from active endocarditis and prophylactic antibiotics may obscure subsequent attempts to identify the causative organism. With this in mind, two or three blood cultures (aerobic and anaerobic) should be considered before antibiotic therapy for those at risk for endocarditis. Patients with a diagnosis of mitral valve prolapse have traditionally been included for treatment with prophylactic antibiotics, but the indication for this is unclear, and antibiotic prophylaxis for uncomplicated mitral valve prolapse is no longer part of the AHA guidelines.62 Kaye63 suggested prophylaxis only for patients who have a holosystolic murmur secondary to mitral valve prolapse. Conflicting results have been reported from the few studies investigating the relationship between I&D of cutaneous abscesses and bacteremia. For example, in 1985 Fine and associates64 concluded that I&D of cutaneous abscesses is often accompanied by transient bacteremia. They compared blood culture results from specimens obtained before and at 1, 5, and 20 minutes after I&D procedures in 10 patients with soft tissue infections. None of the cultures of blood obtained before I&D were positive; however, six patients had at least one positive culture after the procedure. Eleven of the 30 postprocedure cultures yielded growth. In contrast, in 1997 Bobrow and coworkers65 concluded that I&D of a localized cutaneous abscess is unlikely to result in transient bacteremia in afebrile adults. Their study included 50 patients with localized cutaneous abscesses. Blood samples were collected before and at 2 and 10 minutes after I&D. In addition, specimens from the wound were collected after drainage. None of the blood cultures were positive, even though 64% of the wound cultures were positive, primarily for S. aureus. Bobrow and coworkers65 noted that prophylactic antibiotics should be given to patients at high risk for bacterial endocarditis. In a discussion of the differences between these findings and those reported by Fine and associates,64 Bobrow and coworkers65 noted that Fine and associates’ cultures were obtained from indwelling, heparinized IV catheters, a practice that allows ample opportunity for contamination. Furthermore, half the patients in Fine’s group had perirectal abscesses, and if these abscesses involved mucosal surfaces, the risk for bacteremia was potentially increased.64 Immunocompromised patients may benefit from the prophylactic administration of antibiotics in preparation for I&D of cutaneous lesions. In contrast to patients with risks for endocarditis, immunocompromised patients are at risk for septicemia secondary to brief bacteremia. IV drug users have a high incidence of diseases associated with human immunodeficiency virus (HIV),61,66,67 and the treating clinician must anticipate various degrees of immunodeficiency among them. Because no specific standard of care exists, clinical judgment must guide the use of antibiotics in these situations. An approach to individual treatment of recurrent CA-MRSA soft tissue infections is outlined in Box 37-3. Lack of adequate anesthesia is the most common factor limiting I&D in the ED. The current increased use of ED procedural sedation (see Chapter 33) has changed previous OR cases to ones that can be managed well in the ED. If the clinician believes that the abscess cannot be fully incised and drained because of inadequate anesthesia, the patient should be taken to the OR for management under general anesthesia. In addition to limiting proper drainage, it is inhumane and unethical to subject a patient to extreme pain when alternatives are available. A standard suture tray provides adequate instruments if a scalpel and packing material are added (Fig. 37-5). Although sterility is impossible during the procedure, one should avoid contamination of surrounding tissue. Some clinicians prefer to use an obligatory skin scrub with an antiseptic solution, but the value of this step is dubious. Most clinician use nonsterile gloves while draining pus, but practice varies. It is often quite difficult to achieve local anesthesia by direct infiltration because of the poor function of local anesthetic agents in the low pH of infected tissue. Furthermore, distention of sensitive structures by a local injection is quite painful and hence poorly tolerated by most patients. Skin anesthesia is usually possible, but total anesthesia of the abscess cavity itself cannot generally be achieved. If a regional block can be performed (see Chapters 30, 31, and 32), this type of anesthesia is preferred. Alternatively, a field block may be used. It should be noted that infected tissue is very vascular and local anesthetics are therefore absorbed quickly. Strict adherence to maximum safe doses of local anesthetics is required. The skin over the dome of an abscess is often quite thin, thus making skin anesthesia difficult. If a 25-gauge needle is used carefully, one can frequently inject the dome of the abscess subcutaneously. Without moving the tip of the needle, the anesthetic solution spreads over the dome through the subcutaneous layers into the surrounding skin and provides excellent skin anesthesia. If the needle is in the proper plane (best accomplished by holding the syringe parallel rather than perpendicular to the skin), the surrounding skin blanches symmetrically during infiltration without having to reposition the needle (Fig. 37-6, step 2). In an extremely anxious or uncomfortable patient, judicious use of preoperative sedation (see Chapter 33) with IV opioids and sedatives or with nitrous oxide makes the procedure easier for both the patient and clinician. Ketamine, propofol, or a combination of these drugs is a popular option in the ED setting. One should make all incisions conform with skin creases or natural folds to minimize visible scar formation (Fig. 37-7). Care should be taken in areas such as the groin, the posterior aspect of the knee, the antecubital fossa, and the neck so that vascular and neural structures are not damaged. A No. 11 or 15 scalpel blade, held perpendicular to the skin, is used to nick the skin over the fluctuant area, and then a simple linear incision is carried the total length of the abscess cavity (see Fig. 37-6, step 3). This will afford more complete drainage and facilitate subsequent breakup of loculations. Attempting to drain an abscess with an inadequate incision is counterproductive and makes packing changes more difficult. A cruciate or X-shaped incision and an elliptical skin excision are to be avoided in the routine treatment of cutaneous abscesses. The tips of the flaps of a cruciate incision may necrose and result in an unsightly scar (Fig. 37-8). A timid “stab” incision may produce pus but is not generally adequate for proper drainage. The scalpel is used only to make the skin incision and is not used deep in the abscess cavity. Following a standard incision, the operator should probe the depth of an abscess to assess its extent and ensure proper drainage by breaking open loculations (see Fig. 37-6, step 5). An ideal instrument for this procedure is a hemostat, optionally wrapped in gauze (or a cotton swab for small abscesses), which is placed into the abscess cavity and spread and manipulated throughout the cavity (Fig. 37-9). Traditionally, the operator’s gloved finger has been suggested as an ideal way to assess the depth of the abscess cavity and to break up loculations, but this is a potentially dangerous practice that should be avoided unless it is certain that the abscess contains no sharp foreign body. Of particular concern is an abscess caused by skin-popping of IV drugs. These abscesses occasionally harbor broken needle fragments (see Fig. 37-9D and E). In addition, patients who engage in this practice have a high incidence of hepatitis and HIV infection. Clinicians are often surprised at the depth or extent of abscesses discovered during probing. Sharp curettage of the abscess cavity is not usually required and may produce bacteremia. Although tissue probing is generally the most painful aspect of the technique and total local anesthesia is difficult to attain, this portion of the procedure should not be abbreviated. If pain persists, additional local anesthetic can be administered through the cut skin edges and into deeper tissues to provide additional anesthesia (Fig. 37-10A). If the procedure is limited because of pain, use of appropriate analgesia or anesthesia is mandated. Failure to adequately pack the abscess on the first visit makes follow-up packing changes more problematic.
Incision and Drainage
Abscess Etiology and Pathogenesis
Bacteriology of Cutaneous Abscesses
Special Considerations
MRSA
Manifestations of Cutaneous Abscesses
Imaging
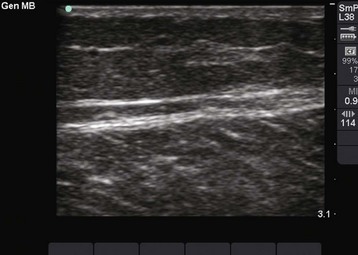
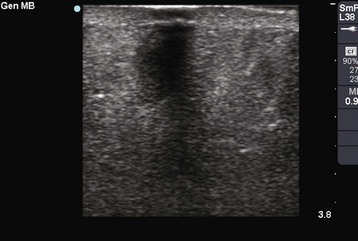
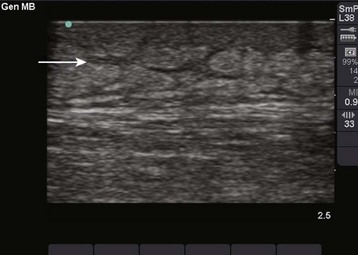
 ULTRASOUND
ULTRASOUND
References:
Laboratory Findings
Indications for and Contraindications to I&D
Prophylactic and Therapeutic Antibiotic Therapy
Therapeutic Antibiotics
Prophylactic Antibiotics
Prophylaxis for Bacteremia in Other Conditions
Recurrent Infections
I&d Procedure
Equipment and Anesthesia
Incision
Wound Dissection
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Incision and Drainage