Chapter 9. Imaging Methods in Cancer Diagnosis
SECTION A Radiography
Jimmy C. Lattimer
KEY POINTS
• Three radiographic views (right and left lateral recumbent and ventrodorsal) of the thorax are essential to assess for pulmonary metastasis.
• Calcified nodules in the lung field are typically granulomas or benign osteomas and should not be misinterpreted as metastatic lesions.
• Radiographic interpretation of bone changes may be more accurate than histopathological evaluation of bone biopsy specimens for diagnosing skeletal neoplasia.
Over the years, the discipline of radiology has expanded in scope to include images generated by ultrasound, computed tomography (CT), magnetic resonance imaging (MRI), gamma cameras, and lasers. Thus, the field is perhaps more appropriately termed imaging and is often referred to in this way. The use of x-rays to project shadows onto film is no longer the predominant method for generating medical images in many radiology departments. Radiographic film is now being replaced by electronic detectors that produce digital images stored in a file on a computer. Nonetheless, radiography is still the quickest and easiest way to evaluate for the presence of a neoplastic process in veterinary patients. It is not the most sensitive or accurate method, but it does provide a large amount of data at a reasonable cost. Frequently, the importance of the radiographic examination is not so much in what is detected, but in what is not detected. For instance, in the evaluation of the thorax in a cancer patient, it is important to not find evidence of pulmonary metastasis. It is also important to not find intercurrent disease such as pneumonia or heart disease. 1
Screening radiographs can and should also guide the use of more sophisticated imaging studies such as CT. For instance, the presence of a nodule in the lung of a cancer patient is frequently viewed as a metastasis—and it may well be. However, a CT scan should be performed to determine the true nature of the nodule and in an attempt to find other smaller nodules not seen on the radiographs. Radiographs of the abdomen provide a more global view of the abdomen than does ultrasound. Diseases of the GI tract in particular are often more easily detected on radiographs, and the presence of GI tract disease on the radiographs can direct attention of the ultrasonographer to a specific portion of the bowel. Mass lesions in the abdomen may be difficult to characterize with respect to organ of origin on ultrasound, but the relative position of other organs to the mass on the radiographs provides guidance in making this determination. Radiographic detection of vertebral lysis in a patient with paresis could indicate that the patient would be more appropriately imaged using CT rather than MRI. These are but a few examples of how radiography can be used to guide the choice of more advanced imaging techniques.
THORACIC RADIOGRAPHS
Three radiographic views of the thorax should be made in all cancer patients. 2,3 The reason for this is twofold. The primary objective of this examination is detection of pulmonary metastasis, disease extension into the mediastinal or hilar lymph nodes, or some other extension of the neoplastic process into the thorax. The secondary objective is to detect any concurrent disease process that would have a negative impact on treatment of the cancer. Examples of the types of diseases that might be detected are heart disease, pulmonary diseases, mediastinal and pleural disease, or diseases of the skeleton. Advanced disease of any of these types could either alter or delay treatment or could obviate it altogether. For example, treatment of a patient with an enlarged heart using doxorubicin may be ill advised or a protracted course of radiation therapy would have little therapeutic value in a patient with advanced pulmonary metastatic disease.
It is essential that the radiographic examination of the thorax consist of both the right and left lateral recumbent views as well as a ventrodorsal (VD) view. 2,3 Because of the recumbent nature of the radiographs generally taken in dogs and cats, there is rapid migration of fluid within the lung to the down side, as well as compression of the down lung lobes by the overlying heart and upper lung. There is also reduced motion of the chest wall and diaphragm on the dependent side, owing to the compressive effects of the animal’s weight. The down side of the diaphragm is also displaced forward by the weight of the abdominal viscera. All of this results in a marked increase in the density of the dependent lung, which can hide not only metastatic lesions but also other lung pathology ( Figure 9-1 ). These effects take place rather quickly and are increased as the animal spends more time on its side before the radiograph is made. Sedation or anesthesia advances the rate and severity of these changes. Radiographs of the thorax taken with an animal under anesthesia should be made with the thorax in a state of forced inhalation by inflating the lungs with a ventilation device. Radiographing the lung field from both sides with a short period of accommodation between allows examination of both sides of the lung field in a relatively aerated state. This facilitates detection of pulmonary lesions, particularly those in the periphery.
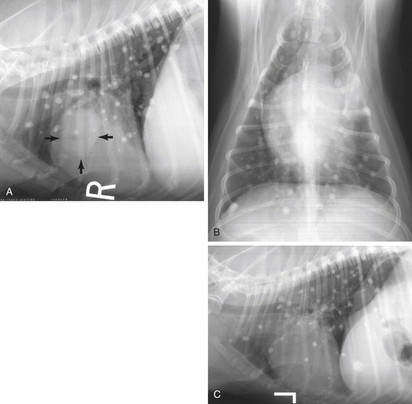 |
| FIGURE 9-1 Right lateral ( A ), ventrodorsal ( B ), and left lateral ( C ) radiographs of the thorax. Multiple, well-defined 3- to 12-mm, smoothly marginated, calcified nodules are seen in all lung lobes. These represent calcified granulomas and are a benign change. The right lateral view also reveals the presence of a 3- × 4-cm moderately circumscribed, soft-tissue opaque mass lesion superimposed over the cranial part of the heart shadow (arrows) . The ventrodorsal view indicates the presence of a poorly defined opacity in the left cranial lung lobe corresponding to the mass lesion seen on the right lateral. The left lateral radiograph ( C ) does not indicate the presence of the mass lesion due to increased opacity of the left side of the lung field by positional atelectasis and fluid shifting. Bronchogenic carcinoma was confirmed after surgical removal of the left cranial lung lobe. |
The orthogonal view should generally be a VD view rather than a dorsoventral view, in order to allow more of the lung field to be seen. The same type of density changes that occur for the lateral positions also occur for the VD view but are generally minimized by the fact that animals are not usually held on their backs for extended periods. Again, anesthesia or sedation will exacerbate the effects. Dorsoventral views are acceptable as orthogonal views and may be preferable if the lateral views detect suspect lesions in the dorsal part of the lung field.
Typical metastatic lesions and other small opacities within the lung are frequently more difficult to detect on the VD view than on the lateral views. This is due to the larger amount of tissue through which the x-ray beam must pass on its way to the film or detector. The heart occupies a relatively larger proportion of the lung field in the VD view, and mediastinal structures obscure the portions of the lung field that cross it. However, the VD view is important for demonstrating that a lesion seen on the lateral view is not located on or in the chest wall (see Figure 9-1 ). A lesion seen over the lung field on orthogonal views is quite likely to actually be within the lung field.
Radiographic detection of metastatic lesions on chest radiographs has a substantial negative impact on the prognosis of a cancer patient. Owners may opt not to proceed with treatment if pulmonary nodules are identified. For this reason it is very important that suspected metastatic nodules be confirmed. Metastatic lesions in the lung field share the general characteristics of any soft tissue nodular lesion in the lung field. Namely, they are single or multiple, round to ovoid, poorly to moderately circumscribed, and of a wide range of sizes and soft tissue in opacity. These characteristics are also those of cysts, abscesses, granulomas and primary neoplasms, and there is essentially no way to specifically differentiate one from the other on the basis of plain radiographs (see Figure 9-1 ). A diagnosis of metastasis should be confirmed by aspiration or at least by demonstrating growth on sequential films. However, the presence of large numbers of nodules of uneven size coupled with the known metastatic potential of the primary neoplasm allows a tentative diagnosis of metastatic disease with a high level of confidence. Likewise, development of new lung nodules in a cancer patient is highly suggestive of neoplasia. However, a diagnosis of metastasis should not be made when the nodules are calcified. 4 Pulmonary metastatic disease, even that arising from bone tumors, essentially never calcifies in dogs and cats, to the extent that it appears calcified on radiographs. On occasion, primary lung tumors may faintly calcify, but even this is rare. Calcified nodules in the lung field are typically calcified granulomas or benign osteomas (see Figure 9-1 ). Thus, any calcified lung lesion must be biopsied to confirm a tentative diagnosis.
SKELETAL RADIOGRAPHS
Radiographs are extremely useful in the diagnosis of osseous neoplasia. It would seem that every oncologist has obtained biopsies of osseous lesions thought to be neoplasia, only to receive a biopsy diagnosis of reactive or inflammatory bone despite a typical clinical presentation. Biopsy only yields a small part of the lesion for histological examination, and bone tumors vary widely in the phenotype of the neoplastic cells from one side of the lesion to the other. There is also usually an inflammatory component in advanced tumors that may obscure the underlying disease. Radiographs depict the entire lesion, and some radiographic lesions very reliably indicate the lesion in question is a neoplasm ( Figure 9-2 ). It has been shown in human oncology that radiographic diagnosis of bone tumors is up to 20% more specific than biopsy. 5 Although improvement in biopsy techniques has closed this gap somewhat, the reliability of a radiographic diagnosis of bone neoplasia by a radiologist in the face of a negative biopsy indicates that the biopsy should be repeated.
 |
| FIGURE 9-2 Dorsal palmar view of the carpus in a dog with a chronic lameness and a lump on the leg. The presence of a large zone of lysis that is indistinctly marginated accompanied by a fragmentation and displacement of the medial radial cortex allows a tentative diagnosis of medullary osteosarcoma with a high degree of confidence. |
SPECIAL PROCEDURES
Radiographic special procedures involving contrast media are still appropriate for diagnosis and characterization of some neoplastic diseases. This is especially true when assessing involvement of the gastrointestinal (GI) and genitourinary (GU) tracts. Small lesions in the GI or GU tracts may be missed by imaging systems with less intrinsic resolution than radiographs, and it may be easier to evaluate extent of involvement on contrast radiographs than on other imaging systems. 6 The functional impact of the disease in these tubular organ systems is easier to assess on radiographs when the variable of anesthesia can be avoided.
LIMITATIONS
Radiographs have historically been used to assess response to therapy or progression of neoplastic diseases. Although this is still appropriate and useful in some cases such as with thoracic or bony lesions, follow-up of other lesions may be more appropriately performed with another imaging modality. Radiography lacks the specificity to evaluate tumor viability and may be quite insensitive to the presence or absence of tumors such as in nasal and brain tumors. Newer nuclear medicine procedures can image tumor metabolism and viability on a time schedule far ahead of that which radiographs indicate simply by reduction or increase in size. Radiography is perhaps the last imaging modality to indicate a response to treatment. This is not to say that radiographic imaging does not have a place in the management of the oncologic patient. However, its role has changed substantially in recent years. This change has occurred dramatically in human medicine but is just as applicable in veterinary medicine.
INTERVENTIONAL RADIOGRAPHY
Interventional radiography is one of the fastest growing fields in imaging. This method uses radiographic imaging, usually fluoroscopy, to guide local non-surgical therapy of neoplastic diseases. 7 Fluoroscopy, in combination with contrast media, can allow the radiologist to guide a vascular catheter into a tumor for local therapy of that lesion. Several such local therapies may be used.
A catheter may be directed into the arterial supply of many tumors. Chemotherapy agents may then be infused directly into the tumor bed, increasing the exposure of the tumor to the agent relative to that of the rest of the body. 8 Tumors with isolated arterial blood supplies such as those of the liver, kidney, thyroid, and spleen are especially suited to this treatment. For example, the arterial blood supply to the liver accounts for only about 10% of the blood supply to the normal liver parenchyma but for greater than 90% of the blood supply of the typical liver tumor. Administration of chemotherapy into the hepatic artery, therefore, should result in a ten-fold increase in drug exposure to the tumor over that seen by the normal liver tissue.
Transvascular embolization of tumors can also be used to control tumor hemorrhage in patients that are poor surgical candidates. A catheter is guided into the vessel feeding the bleeding lesion, and some form of embolus is induced directly into the vessel feeding the tumor. The procedure also defines the blood supply to the tumor by default, which may be of some benefit in planning a subsequent surgical procedure.
One additional method of transvascular therapy of tumors is the introduction of radioactive microspheres into the vasculature of a tumor or organ bearing a tumor. Microspheres made of glass and containing 90 yttrium have been in use for treatment of liver tumors in humans for a number of years. 9 Microsphere therapy may be used for treating any tumor where an isolated vascular supply can be identified. The treatment supplied by this method is twofold: (1) the microspheres deliver radiation directly to the tumor, and (2) they occlude the capillaries of the tumor, thus robbing it of its blood supply. Because the radioactive agent is limited to the tumor, the radiation dose to the lesion can be astronomical relative to the rest of the body or the organ in which the tumor is located. A similar approach to local administration of chemotherapy has also been described.
Fluoroscopy can also be used to guide biopsy procedures to ensure that the sample is obtained from the appropriate part of the lesion (as with bone tumors) or to avoid sensitive surrounding structures (as with lung nodules). Other imaging modalities can be used to do this as well, but in some cases using fluoroscopy is far easier and quicker.
CONCLUSIONS
Although the role of radiography in the diagnosis and management of neoplastic diseases has undergone a dramatic change in the last couple of decades, it remains a mainstay of cancer management. Its repeatability and the quickness with which it can be performed make it the most suitable way to screen for the presence of pulmonary metastasis or suspected skeletal lesions. New and emerging uses of fluoroscopy have added to the scope of radiographic imaging, which holds promise for improved delivery of therapy that increases the impact of therapy while decreasing its side effects. Radiographic imaging will play an important role in the diagnosis and management of cancer for the foreseeable future.
Selected References ∗
D.S. Biller, C.W. Myer, Case examples demonstrating the clinical utility of obtaining both right and left lateral thoracic radiographs in small animals , J Am Anim Hosp Assoc 23 ( 1987 ) 381 – 386 ;
This paper gives good examples of why three views of the thorax should be considered the standard of care when evaluating a cancer patient for disease of the lungs. .
R.P. Moser Jr., J.E. Madewell, An approach to primary bone tumors , Radiol Clin North Am 25 ( 6 ) ( 1987 ) 1049 – 1093 ;
An excellent article describing the approach to evaluating lesions of bone for malignancies. Dr. Madewell is a recognized authority on this subject in human radiology and has written many articles on this subject. .
H. Singh, Interventional radiology in the gynaecological oncology patient , Best Pract Res Clin Obstet Gynaecol 15 ( 2 ) ( 2001 ) 279 – 290 ;
Good article on basic principles and techniques used in interventional radiographic procedures for treatment of cancer .
SECTION B Ultrasound
Stephanie Essman
KEY POINTS
• Sonographic changes are non-specific— biopsy and aspirate !
• Lack of sonographic changes does not rule out neoplasia!
• Target lesions have a high incidence of being neoplasia.
• GI tumors usually result in wall thickening and loss of layering.
Ultrasound is commonly used in veterinary medicine as a complimentary modality to radiographs, especially when evaluating abdominal masses. Advantages of ultrasound include that it is noninvasive, is well-tolerated by the patient, and allows examination of organ parenchyma. The site of origin of a mass can often be determined by ultrasound, and other organs may be evaluated for concurrent abnormalities or metastases. Sometimes, changes noted on ultrasound are non-specific such that neoplastic lesions cannot be distinguished from non-neoplastic diseases without the aid of aspirates or biopsies. In these cases, ultrasound-guided aspirates and biopsies can generally be obtained rapidly and by minimally invasive techniques.
Several patient-related factors can affect the usefulness of ultrasound examinations. Lack of patient compliance, excessive bowel gas, and obesity can all result in a suboptimal examination. Ultrasound is also a highly operator-dependent technique. A thorough examination of the abdomen as well as a basic understanding of ultrasound physics and artifacts is required to perform a high-quality examination.
CHARACTERIZATION OF PARENCHYMAL LESIONS
Echogenicity refers to the relative brightness of a structure. 1 Anechoic structures lack the presence of internal echoes and appear black. When comparing the echogenicity of two organs, the brighter organ is hyperechoic and the darker organ is hypoechoic. 1 Organs that are similar to each other in echogenicity are referred to as isoechoic. Because neoplasia and other types of diseases can result in a change in tissue brightness, knowledge of the relative echogenicity in commonly imaged organs is imperative ( Box 9-1 ). 1
BOX 9-1
COMMONLY IMAGED TISSUE IN ORDER OF INCREASING ECHOGENICITY
• Bile, urine
• Renal medulla
• Renal cortex
• Liver
• Spleen
• Prostate
• Structural fat and vessel walls
• Bone, gas, organ boundaries
Parenchymal lesions of abdominal organs can be characterized as either focal or diffuse. 2 Diffuse disease is characterized by changes in echogenicity. Focal or multifocal abnormalities are characterized by lesions with well-defined margins compared with the surrounding parenchyma. 2 The architecture of these lesions may be cystic, solid, or complex. It is important to remember that sonographic appearance is usually not pathognomic and overlap is seen between benign and neoplastic diseases.
LIVER
Diffuse Disease
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


