Melissa L. Millerick-May
How to Manage Air Quality in Stables
The stable environment has long been implicated as a cause of respiratory disease in horses. As early as the mid-1600s, Gervase Markham described poor air quality in stables as being responsible for some forms of cough in horses. At present, it is common practice to advise owners of horses with recurrent airway obstruction (RAO) or inflammatory airway disease (IAD) to maintain horses at pasture. When this is not possible, owners and stable managers are advised to improve ventilation inside the stable as much as possible and to take action to minimize exposure to dusts from feed and bedding. Unfortunately, behavior modification of the individuals responsible for the care of horses can be difficult once stable management practices have been established. However, with adequate understanding of the problem and focused interventions, stable managers should be able to readily develop and implement a low-dust management protocol that will benefit not only the horses with airway disease but also those free of disease. This chapter focuses on (1) identification of indoor air contaminants commonly found in stables and their relationship to airway disease, (2) identification of the sources of contaminants and common management practices resulting in increased exposures, (3) methods to reduce and minimize exposures, (4) improving ventilation in stables, and (5) managing horses with RAO.
Particulates
Particulate matter (PM) and particulates are the technical terms used to describe dust. The composition and size of particulates dispersed in the air vary. Traditionally, organic dusts were the focus of research pertaining to RAO in horses, specifically dusts from hay. In addition to organic dusts (e.g., mold and plant debris), inorganic dusts are also present and comprise particulates commonly associated with airway disease in humans. Examples of inorganic dusts commonly found in the stable environment include iron and crystalline silica, both known to result in occupational respiratory morbidity in overexposure situations. Particulates in general and silica in particular can induce generation of reactive oxygen species and production of inflammatory cytokines (e.g., interleukin-6, interleukin-8, and tumor necrosis factor-α), and metals such as iron contribute to the toxic effects of such particulates. Diesel particulate materials, recently reclassified as a human carcinogen by the International Agency for Research on Cancer, containing carbon and compounds adsorbed to carbon (i.e., heavy hydrocarbons and hydrated sulfuric acid), and polynuclear aromatic hydrocarbons (solid phase) from vehicle and tractor exhausts may also be present in stables.
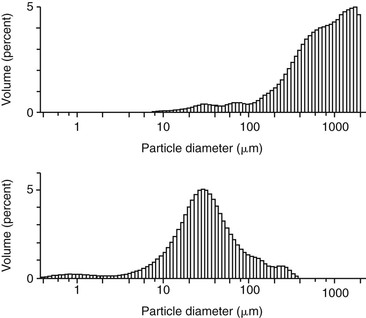
Particle size plays a major role in determining how deeply contaminants penetrate into the lung. Large particles, those visible to the naked eye, are most likely to be trapped by the horse’s respiratory defense mechanisms, such as impaction in the nasal turbinates. Unfortunately, particle size and site of deposition in the airways of the horse have yet to be determined. That said, particle sizes deemed of importance in human airway disease can be used as a guide, with the understanding that, given the relative size difference in the upper airways of the horse compared with those of humans, it is likely that a greater proportion of large-diameter particles have the ability to travel farther into the airways before impaction and sedimentation take place. In humans, only 1% of particles 10 µm in diameter can reach the alveoli, whereas more than 80% of particles 2 µm in diameter do so. To put particle size into context, an average cell in the horse’s body is roughly 10 µm in diameter, a red blood cell is less than 5 µm, and bacteria are about 1 µm. The size of particles contained in a bulk sample of arena footing and the size of particles collected from ledges approximately 3 meters above the ground are depicted graphically (Figure 56-1). Although the bulk of the particulates (by weight) are of the size that would be trapped in the upper airways, the samples taken from ledges are smaller in diameter, with a considerable percentage of the particles less than 10 µm in diameter and a secondary peak of particles about 1 µm in diameter. The diesel particulate materials mentioned previously are generally all less than 1 µm in diameter. In interpreting these panels, it is important to note that it takes many small particles to equal the mass of a single large particle, and these small particles have the ability to stay suspended for long periods of time, thus increasing the opportunity for exposure to those particles that can reach the lower airways. Few studies have been conducted that relate exposure to particulate matter and indices of airway inflammation in horses. Exposure to high concentrations of PM10 (particles ≤ 10 µm in diameter) and PM2.5 (particles ≤ 2.5 µm in diameter) in humans is associated with increased hospital admissions because of respiratory tract disease and increased reports of respiratory symptoms. It was recently demonstrated that high concentrations of PM10 and PM2.5 in stalls are associated with tracheal mucus and increased numbers of tracheal neutrophils in otherwise healthy Thoroughbred racehorses.
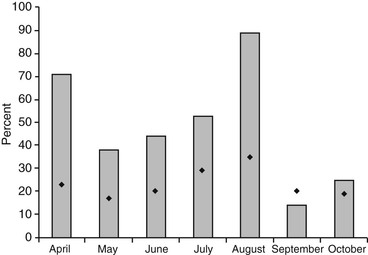
As would be expected, particulate concentrations in stables are highest during times of peak human activity, during seasons with little rainfall, and when it is cold and sources of dilution ventilation (windows and doors) in stables are closed. The concentration of particulates in stalls is related to the prevalence of Thoroughbred racehorses with sufficient tracheal mucus to affect racing performance (Figure 56-2). Because particles associated with airway inflammation in horses cannot be detected by the naked eye yet are of the size that remains suspended in the air for long periods of time, stable managers are likely not aware of the presence of these contaminants that are in sufficient concentration to potentially affect airway health. In addition, it is important to realize that there is no strong correlation between particulate concentrations in the aisle of stables and concentrations of dusts in the breathing zone (i.e., the area around the nostrils) of horses. Therefore stable managers’ perceptions of stable air quality are likely to be inaccurate given that most of their time is spent outside the stall rather than inside the stall where the horse resides.
Irritants
Ammonia is a well-known respiratory irritant commonly encountered in stables. Overexposure to ammonia gas may result in eye, nose, throat, and bronchial irritation; laryngeal edema; cough; bronchospasm; and pneumonitis. The few studies in the literature that report ammonia concentrations in stables investigated air quality in stables or types of bedding that were associated with improved air quality (i.e., reduced ammonia concentrations). In almost every study, however, the ammonia concentrations reported varied with season, bedding type, and stable management protocols (frequency of stall cleaning, how completely stalls were cleaned or rebedded, size, and distribution of ventilation sources). It was not uncommon for ammonia concentrations to reach levels that exceeded published occupational exposure limits, and because horses spend a significant amount of time with their nostrils close to the ground (such as during eating and sleeping), where concentrations are highest, they are potentially exposed to concentrations that are sufficient to induce inflammation.
Source and Dispersion of Airborne Contaminants
Sources of indoor air contaminants are varied. Sources of particulates readily identified by stable managers include feed, bedding, flooring, and arena footing materials. Additional sources include exhausts from tractors or other vehicles left running in the stable, metal fumes liberated by farrier activities, particulates dispersed from surrounding roadways and parking lots, and airborne pollutants from local industry that may enter the stable through open windows and doors. Volatile gases such as ammonia disperse from the point of origin and diffuse into the surrounding airspace.
Dispersion of particulates occurs with both movement of horses and activities of humans. When the horse eats, walks, or rolls, it disperses particulates from feed and bedding into the local environment of the stall. Routine management activities that take place in stables add substantially to the burden. Feeding (throwing hay), cleaning stalls, sweeping and raking aisles, removing cobwebs, maintaining arena surfaces, and grooming horses all disperse particulates of sizes small enough to remain suspended for extended periods of time and are able to reach the lower airways when inhaled. Somewhat recently, blowers have become popular for cleaning floors and other hard surfaces and for removing cobwebs. Besides the inherent physical danger of using high-velocity air to move debris in an enclosed space, small particulates are readily dispersed in large numbers, resulting in high airborne concentrations and greater potential for inhalation exposures than when nonmechanical cleaning methods are used. As would be expected, stables with greater numbers of individuals participating in varied activities simultaneously (e.g., multiple grooms cleaning stalls, raking aisles, and packing hay nets) have higher concentrations of airborne contaminants, compared with stables where only one or two people are working concurrently.
Materials used for racetrack and arena footing vary. Traditionally, soil materials and sand (crystalline silica) were the source materials, with screened varieties specifying the size of individual grains of sand available as an option. Over the years, additional substrates have been added and include pelleted or shredded rubber, wood chips or bark, pulverized concrete, shredded fibers, felts, and others. Consideration has typically been given to the type and depth of footing to be used, on the basis of impressions of benefits with regard to protection to the musculoskeletal system, cost, and ease of maintenance rather than the respiratory health of horses. When footing materials are initially installed, particle sizes tend to be large and do not readily become airborne. Over time and with use, however, footing substrates break down. This is important because it determines the type of contaminant likely to become airborne. For example, sand footing breaks down and liberates crystalline silica, which is known to cause silicosis in overexposure situations. Shredded and pelleted rubber, often from shredded tires, and other materials can liberate metals and dusts coated with hydrocarbons. The more recently developed shredded-fiber–based footings will break down and, depending on the particle size, could result in significant exposures to fibrous dusts that are potentially harmful to the lung: pulmonary immune cells such as macrophages may be unable to completely process fibers, and removal of these materials from the lung can be compromised. Most manufacturers of these products advertise the product as “dust free” if recommended maintenance (application of dust suppressant coatings) and removal or replenishment of source materials is undertaken routinely. At present, there are no reports in the scientific literature describing the potential for respiratory exposures to these types of footing after substrate breakdown.



