49 Histiocytoma
CLINICAL EXAMINATION
In this case a small, dome-shaped tumour with haemorrhagic surface crust was present on the lateral aspect of digit 5 of the left forefoot (Fig. 49.1). The draining lymph node was not palpable.

CASE WORK-UP
A fine-needle aspirate sample was obtained aseptically with a 23-gauge needle. The author’s technique is to insert the needle into the lump and redirect it in and out in several directions and then remove it. A 10-ml syringe containing air is attached to the needle and the contents expressed onto a clean microscope slide by pushing in the plunger. Usually, this method produces a good harvest of cells. The slide is stained with modified Wright’s stain or sent to a cytopathologist. A correct interpretation of the sample is essential to avoid a misdiagnosis, which could lead to major surgery or to other life-threatening treatments.
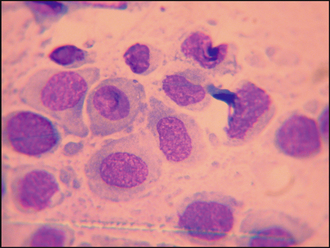
In this case, the fine-needle aspirate revealed a population of mononuclear cells with oval to round nuclei (some with indented nuclear membranes) and pale blue cytoplasm (Fig. 49.2). The cells lacked the granules that one would expect to see with mast cells, thus ruling out a mast cell tumour. Plasmacytomas have a smooth surface that is rarely ulcerated. Cells from a plasmacytoma generally have a more basophilic staining cytoplasm, and the cells show increased anisocytosis (variation in cell size) and anisokaryosis (variation in the size of the nucleus). Sebaceous gland adenomas and hyperplasia yield epithelial cells containing lipid vacuoles, which were not seen in this case, and infectious granulomas would yield large numbers of inflammatory cells such as neutrophils and macrophages that also were not present in this case.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


