, Patricia A. Noguera1 and Trygve T. Poppe2
(1)
Marine Scotland Science, Aberdeen, UK
(2)
Norwegian School of Veterinary Science, Oslo, Norway
Abstract
The oomycetes (fungal-like) occur as primary and secondary agents of infection among wild and farmed salmonids in fresh and sea water. These infections can prove fatal, at least for farmed fish, if preventative measures are not undertaken. Molecular sequencing has improved our understanding of the phylogenetic relationships within this taxonomically diverse group with current evidence indicating these organisms evolved from simple holocarpic marine parasites. This chapter covers the commonly encountered oomycetes infections in salmonids.
Keywords
OomycetesFungusSalmonTrout
Fig. 7.1
Brook trout with severe Saprolegnia infection following handling
The oomycetes (fungal-like) are common and occur as primary and secondary agents of infection among wild and farmed salmonids in fresh and sea water (Fig. 7.1). These infections can prove fatal, at least for farmed fish, if preventative measures are not undertaken. Molecular sequencing has improved our understanding of the phylogenetic relationships within this taxonomically diverse group with current evidence indicating these organisms evolved from simple holocarpic marine parasites. Examples of key infections are summarised in Table 7.1.
Table 7.1
Principal fungal and related oomycete infections of salmonids
Pathogen | Family | Principal salmonid host | Environment |
|---|---|---|---|
Saprolegnia spp. | Saprolegniaceae | All | FW |
Exophiala salmonis, E. psycrophila | Herpotrichiellaceae | Rainbow trout, Atlantic salmon | SW |
Phialophora sp. | Herpotrichiellaceae | Rainbow trout, Atlantic salmon | FW |
Isaria farinosa (Paecilomyces farinosus) | Cordycipitaceae | Atlantic salmon parr | FW |
Phoma herbarum | Didymellaceae | Chinook salmon fingerlings | FW |
7.1 Saprolegnia spp.
Oomycete infections (family Saprolegniaceae) may be commensal or act directly as primary infectious agents and this group, in general terms, is represented by two species, S. parasitica and S. diclina affecting wild and farmed fish at all developmental stages in fresh water (Figs. 7.2, 7.3, 7.4 and 7.5). The presence of superficial cotton-wool-like tufts, particularly on the integument and gills of host fish or eggs, is likely to be the result of Saprolegnia infection. Thin, white or grey threads with circular or crescent-shaped colonies grow by radial extension until adjacent lesions merge (Figs. 7.6 and 7.7). Diseased fish become increasingly lethargic with a loss of equilibrium shortly before death, following lethal haemodilution. Respiratory difficulties may also feature when infection is associated with the gills.




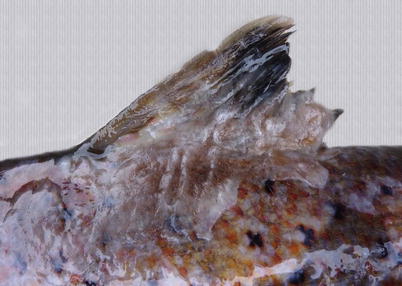

Fig. 7.2
Adult Atlantic salmon returning to spawn in freshwater and infected with Saprolegnia
Fig. 7.3
Saprolegnia infection on head and at the base of pectoral fins of a wild adult Atlantic salmon
Fig. 7.4
Extensive Saprolegnia infection comprising head, ventral body and tail in wild adult Atlantic salmon
Fig. 7.5
Spawning whitefish with patchy Saprolegnia infection on head, body flank and fins
Fig. 7.6
Adult Atlantic salmon with extensive Saprolegnia infection on dorsal fin and adjacent skin
Fig. 7.7
Atypical circular infection on body flank of spawning wild Atlantic salmon
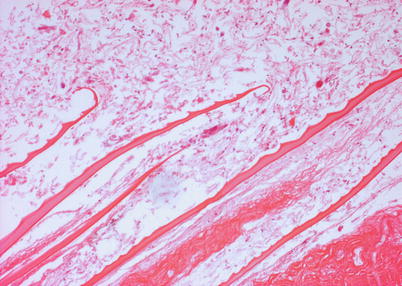
Microscopic examination shows the characteristic filamentous, coenocytic mycelium of non-septate hyphae with many zoosporangia. An early infection comprises rapid degenerative changes in the muscle resulting in a diffuse oedema. As the infection radiates from the focus of infection, more of the epidermis is destroyed, and consequently hyphae can penetrate the basement membrane, with growth continuing into the dermis, hypodermis and musculature (Fig. 7.8). Thrombi are frequently observed in blood-vessels as a result of the penetrating hyphae. There is loss of integrity of the integument and oedema of the hypodermis accompanied by marked myofibrillar degenerative changes. Severe infection causes swelling in the inter-myotomal connective tissue, loss of nuclei and a minor host reaction. More aggressive lesions show deeper myofibrillar and focal cellular necrosis, spongiosis or intracellular oedema and ultimate sloughing of the epidermis.