36 Feline constipation and megacolon
Initial presentation
Tenesmus, haematochezia and abdominal distension
Signalment: 8-year-old, female neutered Devon Rex cat, body weight 2.5 kg
Physical examination
The cat appeared slightly thin (body condition score 3/9) and had a distended abdomen (Fig 36.1). Her hydration appeared adequate and mucous membrane colour was pink with a capillary refill time of 2 seconds. Thoracic auscultation revealed a Grade I to II/VI systolic murmur, with point of maximal intensity at the left sternal border. No pulse deficits or arrhythmias were detected. Respiratory rate was mildly increased at 30 breaths per minute, attributed to stress, as no abnormal lung sounds were detected. Abdominal palpation revealed a large colon, filled with hard faeces and a moderately distended bladder.

Problem list and discussion of problems
Differential diagnosis
Differential diagnoses for constipation include:
Case work-up
Imaging
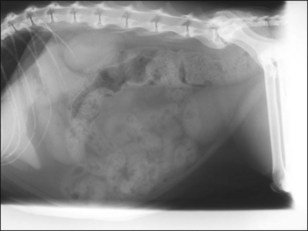
Abdominal radiography showed impaction of the transverse and descending colon with faeces (Fig 36.2). In addition, ventral spondylopathy was present at the lumbosacral junction. Two views were taken to fully evaluate narrowing of the pelvic canal.
Follow-up
Over the following 18 months the cat required increasing doses of lactulose and cisapride and micro-enemas with sodium alkylsulphoacetate on three occasions. The cat subsequently presented after having not defecated for 4 days. She also again had a poor appetite and was lethargic. Further radiographs were obtained which showed a grossly dilated impacted colon (Fig 36.3) and as the condition was no longer responding to management a diagnosis of idiopathic megacolon was made.




