F
Feeding Tube Placement: Esophagostomy Tube 
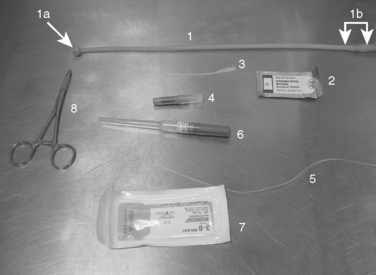
EQUIPMENT, ANESTHESIA
• Long polypropylene catheter (optional). If used, it should be as long as, or longer than, the feeding tube.
• Bandage material: sterile dressing, roll gauze, dry adherent wrap (e.g., Vetrap or Elastikon-type)
PREPARATION: IMPORTANT CHECKPOINTS
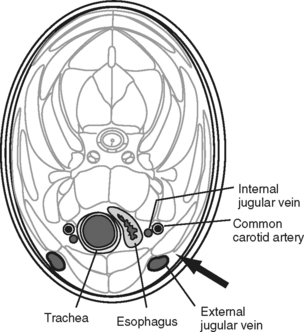
Familiarization with the locations of the great vessels:
• When preparing the site of esophageal tube placement, it is essential to distend the jugular vein periodically by occluding it manually at the thoracic inlet. This allows visualization of the jugular vein to prevent vascular trauma during tube placement.
POSSIBLE COMPLICATIONS AND COMMON ERRORS TO AVOID
PROCEDURE
• Clip and aseptically prep the midcervical region: most or all of the left side of the neck is prepared. In smaller patients (cats, small dogs), the area extends from the angle of the mandible to the thoracic inlet and covers the entire left side of the neck from dorsal to ventral midlines; however, in larger dogs, a somewhat smaller relative area (e.g., 15-cm square) is sufficient.
• Trim the tube to the correct length:
○ Determine the proper length of the feeding tube by measuring the distance from the midcervical region (midpoint between angle of mandible and thoracic inlet) to the seventh or eighth intercostal space (ICS). In addition to this measured length, add approximately 6 cm of extra length to the measurement to account for the segment of tube that will remain outside the animal.
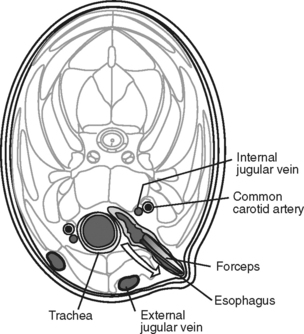
• Introduce curved forceps into the oral cavity, orienting the tips of the forceps pointing up (left lateral direction).
○ Advance the forceps caudally into the oral cavity such that the forceps tips enter the esophagus and can be felt through the skin.
○ Palpate the desired region (the left hand orients the forceps deep into the animal’s mouth, and the right hand palpates the forceps tips through the esophagus and skin) until forceps tips are in the proper location:
▪ Proximal placement of the tube (pharyngeal) is a common error caused by incomplete insertion of the forceps. The tips of the forceps should be caudal to the point at which the maxillary and sublingual veins converge into the external jugular vein and must be caudal to the entire larynx.
▪ Avoid placement that overlies the jugular vein. Raising the jugular vein by applying pressure at the thoracic inlet allows it to be more clearly visualized and thus avoided. This should be done repeatedly when identifying the site of tube insertion and preparing to make the incision.
• Elevate (lateral pressure, upward away from the table) the distal part of the forceps, and again confirm a proper location.
• Force the forceps tips through the esophageal wall and skin by incising over the instrument tips with a scalpel. The distal-most tips of the forceps should now have emerged through a snug, very small (a few millimeters) incision in the skin and lateral esophagus.
• Open the forceps tips slightly, just enough to grasp the distal tip of the feeding tube. Close the forceps on the feeding tube tip, and draw the feeding tube out with the forceps (cranially) through the opening and most of the way out the oral cavity, leaving only about 6 cm of tube protruding through the skin.
POSTPROCEDURE
• Postprocedure radiographs will ensure proper placement prior to anesthetic recovery. The tube should extend to the distal esophagus but should not enter the stomach.
• Most animals tolerate these feeding tubes well, but some may need an Elizabethan collar to prevent damaging the tube.
• Feedings may be started as soon as the animal recovers from anesthesia, and the tube may be removed at any time. Removal generally does not require anesthesia or sedation, and the stoma heals by second intention.
ALTERNATIVES AND THEIR RELATIVE MERITS
• Nasoesophagostomy tube: typically only liquid diets (much smaller in diameter); however, the tube can be placed without general anesthesia. Animals generally do not tolerate this type of tube as well as other tubes.
• Percutaneous endoscopic gastrostomy (PEG) tube: can place a larger-diameter tube and provide bolus feedings. Appropriate in cases of esophageal disease, where esophagostomy tubes are not well tolerated. Unlike esophagostomy tubes, gastrostomy tubes cannot be used for 24 hours post placement during healing of the stoma and should not be removed until after 7 days post placement.
Feeding Tube Placement: Nasoesophageal and Nasogastric 
CONTRAINDICATIONS
• Animals with severe pharyngeal, laryngeal, or esophageal physical or functional abnormalities (e.g., severe megaesophagus, esophageal surgery, or perforation, absent cough or gag reflex)
PREPARATION: IMPORTANT CHECKPOINTS
• Select the largest tube that will be able to pass through the nares. Approximate guidelines: puppies and kittens, 3 Fr gauge; cats and small dogs, 5 Fr; larger cats and dogs, 8 Fr or bigger; giant dog breeds, typically 12-18 Fr. If the tube diameter is too small, even the most dilute solutions will not be able to pass through the tube.
• Premeasure and mark the length of the tube that should be passed. For nasogastric intubations, the tube is measured from the nostril to the ninth intercostal space (ICS); for nasoesophageal feeding, the tube is measured up to the sixth ICS.
POSSIBLE COMPLICATIONS AND COMMON ERRORS TO AVOID
• Excessive lidocaine administration in cats and possibly smaller dogs (toxic dose [topical]: 4 mg/kg)
PROCEDURE
• Elevate the nose so the animal is looking at the ceiling, and with the animal’s mouth closed, instill approximately 0.25-0.5 mL lidocaine in each nostril, depending on the size of the animal. Note: Remember toxic dose in cats. It is helpful to time the instillation to when the animal is inhaling, so as to minimize the amount of anesthetic blown or sneezed out of the nares. Both nostrils are anesthetized at this time to avoid delay if it becomes necessary to use the other nostril. The head and restraint are released while allowing lidocaine to take effect: typically 1-2 minutes.
• The tube is directed ventromedially into the nostril and passed via the ventral meatus. In dogs, the nostril can be pushed dorsally to assist easy passing of the tube.
• The tube is advanced up to the premeasured mark. Avoid extending the neck, because this will increase the risk of tracheal intubation. Slight flexion of the neck will help the animal to swallow the distal end of the tube and facilitate proper placement.
• Check correct placement of tube in the esophagus or stomach:
○ Attempts to aspirate air from the tube with a syringe will create negative pressure if the tube ends appropriately in the esophagus. If air is easily withdrawn during aspiration from the tube, it is likely in the pharynx or trachea.
○ Injecting air through the tube should create gurgling sounds on auscultation of the stomach if the tube was successfully placed into the stomach.
○ Radiographs may be taken of the cervical and thoracic esophagus to visually confirm location of the tube.
○ Note: Do not check tube placement by injecting water into the tube. Theoretically, an animal will cough if the tube is placed in the trachea, but some animals may be too weak to cough; in cats in particular, coughing is a very poor indicator of tube placement, because the majority of cats will not cough even when the tube is intratracheal.
• The tube can either be sutured or glued into place. The first point of attachment to the skin is as close to the nares as possible. Additional sutures or glue should be placed on the dorsum of the muzzle or on the cheek. Make sure to avoid the whiskers in cats to prevent irritation.
• Some animals do not tolerate the tubes because of irritation, and the use of an Elizabethan collar can be indicated depending on the temperament of the animal.


POSTPROCEDURE
• Regularly flush the tube with a volume of water equivalent to or greater than the volume of the tube itself. Doing so helps to avoid blockage and is indicated especially prior to and immediately after administering food.
• A prokinetic (e.g., metoclopramide) could be used to assist with the functioning of the lower esophageal sphincter to minimize the risk of esophageal reflux.
ALTERNATIVES AND THEIR RELATIVE MERITS
• Alternative feeding tubes could be placed with minor surgery and short general anesthesia (e.g., a percutaneous endoscopic gastrostomy [PEG] tube or esophagostomy tube) or major surgical procedures requiring long general anesthetics (e.g., gastrostomy and jejunostomy tubes).
• These tubes are often indicated for animals in which nasoesophageal and nasogastric tubes are contraindicated (see Contraindications, above).
Feeding Tube Placement: Percutaneous Endoscopic Gastrostomy (PEG) 
EQUIPMENT, ANESTHESIA
• Sturdy suture material (e.g., polyamide, nonabsorbable, 0 or larger gauge), at least 1 m (3 ft) long for most animals and up to 1.5 m (5 ft) for large dogs
PREPARATION: IMPORTANT CHECKPOINTS
• Preparation of the animal: the left side of the abdomen is shaved and aseptically scrubbed. The animal is anesthetized and placed in right lateral recumbency.
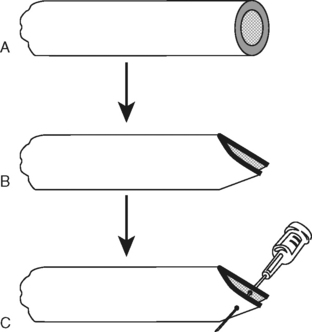
• Preparation of the Pezzer tube:
○ The 3-mm blunted protuberance (“nipple”) at the extremity of the ampulla (“mushroom head”) of the Pezzer tube should be cut off with scissors to facilitate the passage of food. Note: The ampulla/mushroom head itself is not cut; only the small protuberance on it is cut, creating an additional end hole in the ampulla. It is also important to avoid cutting into the adjacent end holes in the ampulla, which would weaken the ampulla’s structure.
○ The proximal flared end (the non-mushroom end) of the Pezzer tube should then be cut just prior to the wider cylindrical extremity (i.e., cutting off the most proximal 3-4 cm of tube; Panel A). The cut segment is important and must not be discarded.
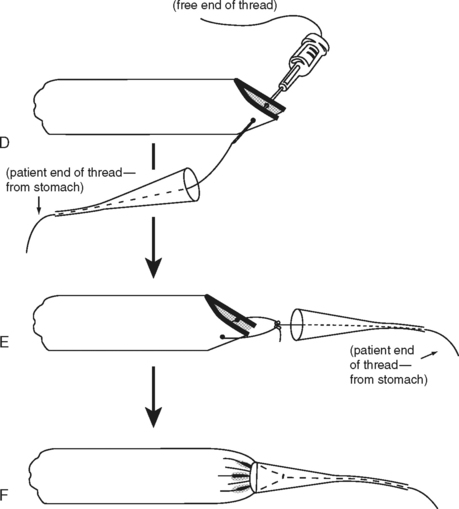
○ Next, trim this same proximal extremity of the Pezzer tube into an arrow shape (Panel B) to allow fitting this end inside the wide extremity of a tomcat catheter (Panels C-F). The 16-gauge needle should then be passed through the walls of this end.
○ The 3- to 4-cm cut segment is kept to create a flange which will ultimately stabilize the tube: using a #11 scalpel blade, make a 5-mm stab incision in the midbody of the tube segment. Repeat the stab incision on the opposite side of the tube segment such that two parallel and longitudinal 5-mm incisions are created in alignment to each other in the middle of the segment. These transverse incisions will allow passage of the Pezzer tube through them such that the flange prevents inward migration of the tube when the animal is awake and mobile.
POSSIBLE COMPLICATIONS AND COMMON ERRORS TO AVOID
• The thread needs to be sturdy because otherwise it may break during the pulling of the Pezzer tube through the gastric and abdominal wall.
• The ampulla of the Pezzer tube may be blocked at the level of the gastroesophageal sphincter. A firmer pull will allow the ampulla to pass this obstacle. Note: It is essential to brace this traction on the tube with counterpressure at the level of the body wall. If pulling the Pezzer tube into place with the right hand, the clinician’s left thumb and forefinger are on the body wall, adjacent to the tube, and are exerting counterpressure to make sure the ampulla stops at the stomach wall and does not come out entirely.
• The Pezzer tube must be left in place for at least 2 weeks to allow fibrous tissue to surround the portion of the tube between the stomach and the abdominal wall, thereby sealing it off from the abdominal cavity. This is important for the safe removal of the Pezzer tube and minimizes the risk of peritonitis.
• The incisions in the flange need to be long enough to avoid creating a stricture of the Pezzer tube.
PROCEDURE
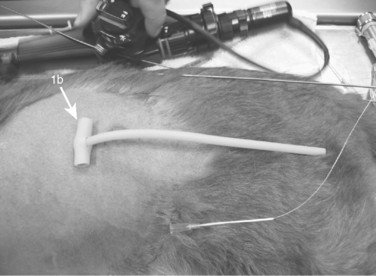
• The endoscope is introduced into the stomach, and the extremity of the endoscope should be pointing toward the left side of the antrum. The light at the endoscope tip should be visible through the skin.
• The extremity of the over-the-needle IV catheter is then introduced into the gastric lumen through the skin, aiming for the light of the endoscope.
• Once the catheter is introduced into the stomach, the stylet is removed. The thread can then be introduced through the catheter into the stomach.
• With the endoscope, the extremity of the thread inside the stomach is grabbed using the biopsy forceps of the endoscope; thread, biopsy forceps, and endoscope are pulled outside all together through the esophagus and the mouth. Note: Ensure that the proximal end of the thread is kept outside (e.g., clamp it with a mosquito hemostat) to avoid the whole length of the thread being pulled through.
< div class='tao-gold-member'>
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


