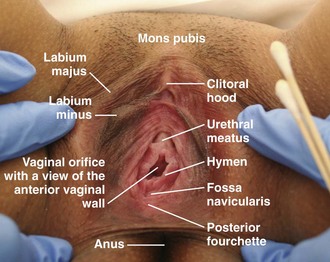
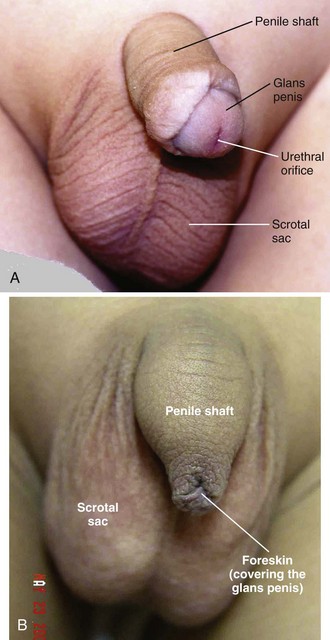
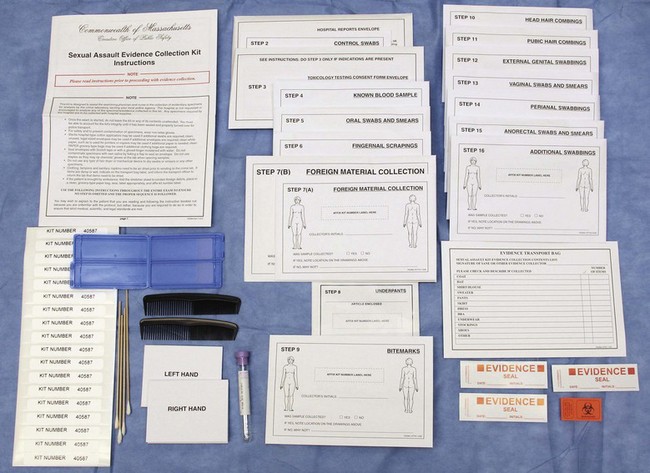
Chapter 58 The majority of sexually assaulted individuals never report the crime to anyone, and only one third of sexual assaults are reported to law enforcement. In many cases, after contact with law enforcement, sexual assault victims are taken to the emergency department (ED) for evaluation, examination, and treatment. Sexual assault victims may also go to the ED without prior contact with law enforcement. In 2009, sexually assaulted patients accounted for approximately one tenth of all assault-related visits to the ED by female patients.1 Some sexual assault victims will cooperate with police investigations, but others will not. Federal legislation guarantees all victims the right to a forensic examination and treatment of sexual assault regardless of their cooperation with legal investigation or their desire to initially pursue prosecution.2 Some states require medical personnel treating sexual assault victims to report the assault to local law enforcement, whereas others forbid such reporting without patient consent. Clinicians must know their own state laws regarding such reports. Sexual assault refers to any sexual contact between one person and another without appropriate legal consent.3 Physical force may be used to overcome the victim’s lack of consent, but this is not mandatory to prove assault. Coercion into sexual contact by intimidation, threats, or fear also defines sexual assault. State laws differ slightly on the definition of exact acts that constitute sexual contact and on which populations are unable to give legal consent. In general, persons under the influence of drugs or alcohol, minors, and those who are mentally incapacitated are considered unable to give consent for sexual contact. ED personnel must secure patient privacy and designate a separate area for the care of sexually assaulted patients. If medically and logistically possible, interviews should be conducted in a private room separate from the examination room. EDs often have such an area, frequently called the “grieving room” or the “family room.” Law enforcement or other governmental agencies may provide examination kits for the collection of forensic evidence from victims (Fig. 58-1). These kits should be available in the ED and the staff should be familiar with them. If such kits are not provided by local sources, hospital staff may need to assemble their own kits from material found in most EDs. Alternatively, private companies assemble and sell such kits (www.lynnpeavey.com or The Lynn Peavey Company, PO Box 14100, Lenexa, KS 66285-4100). Prepared kits save a tremendous amount of nursing and clinician time when a victim comes to the ED. A checklist of local requirements for sexual assault examination should be included in the kits and serves as a reminder for all the medicolegal procedures to be completed. Elements of the victim’s history should help in deciding which potential samples to collect. For example, sperm may be recovered from the cervix for up to 12 days after intercourse and from the vagina for up to 5 days (Table 58-1).4 If the victim had voluntary intercourse 48 hours before the examination and was sexually assaulted 3 hours before the examination, obtain samples from both the vagina and the cervix and keep the two types of specimens separate. Taking a careful history makes it possible to perform an appropriate examination given these two separate events. In general, cervical swabs should be collected in addition to the usual vaginal swabs if the time between assault and examination is longer than 48 hours or if intercourse with a different person took place within a few days of the assault. Some experts advocate cervical samples in all cases that will involve speculum examination because of greater forensic yield. TABLE 58-1 Maximal Reported Time Intervals for Sperm Recovery From Marx J, ed. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 6th ed. Philadelphia: Elsevier; 2006. After the patient disrobes and is placed in a gown, examine her body for signs of trauma and foreign material. Uncover one part of the body at a time to examine and then carefully re-cover it. This allows the victim to retain some modesty during the examination. Important areas for evaluation are the back, thighs, breasts, wrists, and ankles (particularly if restraints were used). Even in the absence of ecchymosis, note tender areas during the examination. Evidence from the physical surroundings of the assault can occasionally be found in the hair or on the skin. Retain such material as evidence. Document areas of trauma and evaluate further (e.g., with radiographs) as indicated by the type and extent of injury. Approximately 10% to 67% of sexual assault victims display bodily injuries.3 Document these injuries because they correlate significantly with successful prosecution of perpetrators.5 Bodily evidence may range from abrasions to major blunt and penetrating trauma. If the victim has not bathed, bodily evidence in the form of dried semen stains may be visible on the hair or the skin of the victim. In a darkened room, dried semen (and, unfortunately, many other substances) on skin may fluoresce under examination with shortwave light, such as that produced by a Wood lamp or an alternative light source, but may also be noticed equally well by its reflective appearance under regular room lighting.6,7 Use moistened swabs to collect potential dried secretions; then air-dry them thoroughly and preserve as evidence. Fragments of the assailant’s skin, blood, facial hair, or other foreign material from the assault site may be trapped beneath a victim’s fingernails. Obtain fingernail scrapings by cleaning under a victim’s nails with a toothpick or small swab or by cutting the nails closely over a clean piece of paper. Fold the toothpick and debris into the paper, place it in an envelope, and package it with the other specimens. If indicated by the history, inspect the oral cavity closely for signs of trauma and collect evidence if indicated. Mouth injuries from forced oral copulation include lacerations of the labial or lingual frenulum, mucosal lacerations, and abrasions. Injury to the lips is often produced by the victim’s own teeth as her lips are forced inward by forced oral penetration with the perpetrator’s penis. Potential injuries to the posterior pharyngeal wall and soft palate include petechiae, contusions, and lacerations (Fig. 58-2). Document these injuries at the initial examination because mucosal injuries heal quickly and may not be present hours or days later. Collect potential evidence with swabs rubbed between the teeth and the buccal mucosa on both the upper and lower gingival surfaces bilaterally. Spermatozoa have been identified in oral smears for hours after the attack despite brushing the teeth, using mouthwash, or drinking various fluids and may provide valuable evidence up to 12 hours after examination.8,9 Collect any foreign material (e.g., hair) to include as potential evidence. During the oral inspection, local law enforcement may request that examiners collect buccal cell swabs to provide the crime laboratory with a sample for victim DNA reference. Significant hair transfer occurs in less than 5% of assaults.10 For the small minority of cases in which foreign suspect hairs must be compared with the victim’s hair, a sample pulled from the victim may be desired. Although pulling the patient’s hair from the roots may provide the best sample, this collection method is painful, considered insensitive, and not recommended by these authors during the initial evaluation. These hairs will rarely be needed because the vast majority of cases are never adjudicated and those that are rarely concern this type of evidence. A victim can provide the hairs at a later time, if needed, and frequently the victim is willing to pluck the hairs herself at that time. Genital examination of a sexual assault victim differs considerably from most ED pelvic examinations. First, perform a careful evaluation of the vulva and vaginal introitus for signs of trauma. The techniques of separation and traction move the tissues most likely to suffer injury into view. In performing separation, examiners use both hands to separate the labia laterally in each direction and inspect the posterior fourchette and vaginal introitus. Similarly, in performing traction, examiners use both hands to hold each labium majus and apply gentle inferior labial traction (i.e., toward the examiner); this gives a much-improved view of the hymen, especially in prepubertal females (Fig. 58-3). If the examiner fails to perform these maneuvers, traumatic genital injuries may be missed. Familiarity with female (Fig. 58-4) and male (Fig. 58-5) genital anatomy, including all terms, is important for accurate descriptions. Although most novice examiners concern themselves with detecting injuries to the hymen, the majority of sexual assault–related vaginal injuries occur to the posterior fourchette (Fig. 58-6).11 In fact, hymenal injuries are rare in sexually active adult women and are more commonly observed in sexually inexperienced adolescents12,13 (Fig. 58-7). More uncommon injuries to the vaginal walls and cervix may be discovered during the speculum examination. Reported rates of genital injury in forensically examined victims range from 6% to 20% without colposcopy to 53% to 87% with colposcopy.11–13 Most importantly, examiners must be cognizant of the fact that completely normal findings on genital examination remain consistent with forced sexual assault. In fact, a study of more than 1000 sexual assault victims found that almost half of all victims with forensic evidence positive for sperm had no genital injury.14 Teixeira first described the use of colposcopy for documentation of sexual assault in 1981.15 Although it is not readily available nor a standard of care in most EDs, the use of colposcopy has revolutionized the documentation of injury. The colposcope provides magnification, a bright light source, and usually permanent documentation of injuries in the form of still images or video (mainly in digital format but occasionally traditional film). In one small study the colposcope increased the rate of detection of genital injury from 6% to 53%.16 Colposcopes with photo or video attachments provide excellent photographic documentation for the court and allow review by expert practitioners for court testimony without subjecting the victim to reexamination (Fig. 58-8). Experienced sexual assault examiner programs are increasingly using high-quality digital single-lens reflex cameras mounted on a tripod to obtain excellent images that are indistinguishable from those obtained with colposcopy. ED practitioners may have access to such equipment. Colposcopically visible injuries have also been described in adolescent women after the first consensual intercourse; hence, genital injury does not always correlate with nonconsensual vaginal penetration.17 Conversely, totally normal findings on genital examination by colposcopy are often found after sexual assault. Even in sexually inexperienced adolescents, forced penetration can occur without leaving discernible genital injury.17 Although previous sexual experience by the victim decreases the likelihood of finding genital injury, experts cannot fully explain the reasons why some rape victims sustain measurable genital injury whereas others do not. Protocols for collection of evidence vary by legal jurisdiction. Many sexual assault evaluation centers have abandoned the cumbersome kits used in the past and substituted simple collection methods that concentrate on important and usable legal evidence. The following discussion draws from the model protocol suggested by the state of California and the American College of Emergency Physicians manual.3 Obtain standard specimens during inspection of the external genitalia, rectum, vagina, and cervix. Lubricate the speculum with warm water rather than other lubricants because of the potential spermicidal activity of lubricants. However, if lubricants are inadvertently used, the potential for corruption of DNA evidence should be negligible.18 Generally, the specimens collected will be determined by victim’s history and local protocol, but they may include any of the items listed in Box 58-1 and shown in Figure 58-9. Some protocols recommend that examiners make a wet mount of one swab from the vaginal pool and look at it under the microscope for the presence of motile sperm. Because of rapid cell death, studies have shown a negligible chance of finding motile sperm from a vaginal wet mount more than 8 hours after intercourse.19 Furthermore, in complying with the Clinical Laboratory Improvement Amendments of 1988, ED practitioners in the United States rarely have sufficient access or experience with microscopy to make this step a routine recommendation. Several swabs from the vaginal pool (including the one used to make the wet mount, if done) and the external genitalia should be obtained and then applied over clean slides for a dry mount. These slides should be allowed to air-dry and then labeled; all swabs and slides should be packaged in paper envelopes for the local crime laboratory. Some EDs maintain specific equipment (i.e., a Dry Box) to aid in the drying of specimens; in others, the swabs and slides must be left out until completely dried. Crime laboratories may also request collection of a vaginal washing. For this procedure, insert 5 mL of sterile (but not bacteriostatic) water or saline into the vagina and then remove it. Place the washing in a sealed container (such as those used for urine collection or a red-topped blood tube). In addition, collect cervical swabs if the time from assault to examination (the postcoital interval) is longer than 48 hours or if there is a history of recent consensual intercourse as well. The crime laboratory may recover sperm from cervical specimens up to 12 days after coitus.3 Guidelines from the Centers for Disease Control and Prevention (CDC) suggest obtaining a cervical, rectal, or oral specimen for culture or polymerase chain reaction (PCR), or both, for Chlamydia trachomatis and Neisseria gonorrhoeae. However, the majority of SART programs in the United States do not routinely perform these tests.20 STD testing during sexual assault examination can detect only infection before the assault and provides no meaningful information for the crime laboratory. In addition, routine prophylactic treatment with antibiotics effective against N. gonorrhoeae and C. trachomatis makes detection of these preexisting infections superfluous; however, clinicians might want to consider obtaining samples for culture from child victims, in whom the presence of an STD would be indicative of previous sexual contact. Toluidine blue dye is a nuclear stain, also used for cancer detection and mast cell staining, that highlights areas of injury. It adheres to areas denuded by abrasions and lacerations where the epidermal layer of nonnucleated cells has been removed (Fig. 58-10). The underlying nucleated cells take up the dye. Although it is not a uniform standard of care and unavailable in many EDs, the dye can enhance the examiner’s ability to visualize and photographically document more subtle genital injuries (see Fig. 58-6). Genital lacerations may provide corroborating evidence of nonconsensual intercourse, or at least sexual activity. To outline injuries, apply a 1% aqueous solution of toluidine blue dye to the perineum and wipe the excess dye off with a cotton ball moistened with lubricating jelly. A swab containing the dye is commercially available. After the excess dye is removed, any areas that retain the stain signify a disruption in the epidermis, most likely injury. Separate any folds of the area and carefully examine them to avoid missing injuries. Ideally, apply the dye before speculum examination to eliminate the possibility of iatrogenic injury. The procedure is described in Figure 58-10 and Box 58-2. In one study, use of toluidine blue dye increased the injury detection rate from 16% to 40% in women without the use of colposcopy21; however, injuries detected with the aid of toluidine blue dye are not 100% specific for sexual assault because such injuries have also been found after consensual intercourse, especially in adolescents.22 Box 58-2 Toluidine Blue* Staining of the Perineum to Detect Microabrasion† 1. Collect all external genital specimens as indicated by examination before application of the dye.‡ 2. Before speculum examination or anoscopy, apply 1% toluidine blue to the entire vulva (labia majora, labia minora, posterior fourchette, perineal body, and perianal area). The anus may also be stained. Do not use dye in the vaginal vault or mucous membranes. 3. Allow it to dry for approximately 1 minute. 4. Remove excess dye with water-soluble lubricant by gently blotting the area until the excess dye is removed. 6. Photograph the area if indicated.
Examination of the Sexual Assault Victim
Definitions
Evaluation and Treatment of Patients Suffering From Sexual Assault
History
BODY CAVITY
MOTILE SPERM
NONMOTILE SPERM
Vagina
6-28 hr
14 hr-10 days
Cervix
3-7 days
7.5-19 days
Mouth
—
2-31 hr
Rectum
—
4-113 hr
Anus
—
2-44 hr
Physical Examination
General Body Examination
Oral Evaluation
Pubic Hair Samples
Colposcopy
Forensic Evidence Collection
Genital Testing for STDs
Perineal Toluidine Blue Dye Staining
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Examination of the Sexual Assault Victim