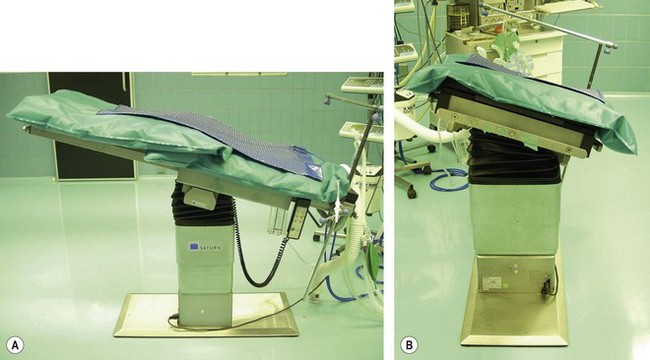
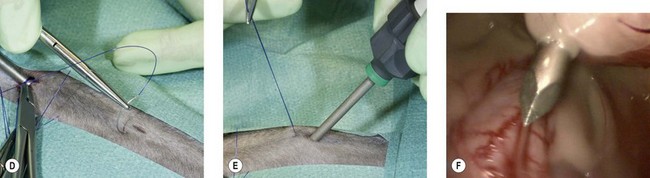
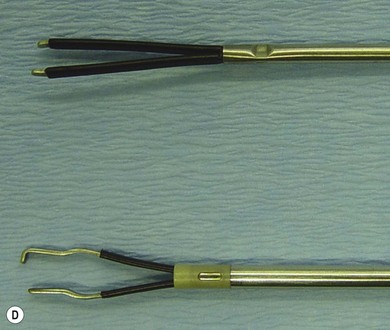
Chapter 24 Rigid endoscopy enables visualization of the abdominal cavity in a minimally invasive approach.1,2 Laparoscopy and celioscopy are terms used for the abdominal cavity and thoracoscopy for the chest. Laparoscopic surgery is performed with special instruments through small-diameter access-points (portals) in the abdominal wall (Fig. 24-1). Apart from the advantage of minimally invasive access causing less incisional trauma, the use of an optical laparoscope enables a close-up view of abdominal tissues, improving visibility compared to open surgery. Thus, laparoscopy can improve access to abdominal tissues without requiring extensive manipulation (e.g., exteriorization of tissues) resulting in reduced pain and trauma of tissues compared to open surgery. In human evidence-based medicine, laparoscopy has become the preferred approach for a growing number of surgical procedures, including cholecystectomy,3 ovariectomy,4 and appendectomy.5,6 Likewise, laparoscopy is increasingly used in veterinary medicine and surgery,7–9 including in smaller animals such as reptiles, ferrets, and rodents.10,11 Several advantages of laparoscopic surgery compared to open surgery that have been described for humans, have also been reported in dogs, including reduced peri- and postoperative pain,12–14 less postoperative adhesion formation,15–17 a shorter convalescence period and faster return to normal activity level,18–21 and reduced surgery-induced physical stress and inflammatory response.13,14,16,22–25 In cats, descriptions of laparoscopic procedures are sparse and include exploratory laparoscopy for observation of abdominal organs,1 biopsy of abdominal organs,26–28 ovariectomy,29–31 ovariohysterectomy,32 and abdominal cryptorchidectomy.33,34 Few case reports of other procedures exist.35,36 The smaller size of cats and their different conformation of skin and abdominal wall, compared with dogs, require a different approach to minimally invasive surgery in this species. However, adapting to these differences enables minimally invasive surgical approaches similar to those in other species to be performed, with comparable advantages. The main disadvantages of laparoscopic surgery are the associated costs of investment in equipment, specific anesthetic requirements, and the need for an assistant, especially in more advanced procedures. Furthermore, the acquisition of minimally invasive surgery skills is known to be associated with a distinct learning curve, requiring considerable training. Practice on low-cost box-trainers or cadavers can be very useful,37,38 particularly in cats with their relatively small abdominal cavity. However, the anatomy of the abdominal wall in cats also has advantages that will be discussed later. The operating room is set up according to the surgical procedure to be performed. Ideally, the surgeon, the operating field, and the monitor displaying the image of the laparoscope are positioned in a straight line. This so-called coaxial set-up maximizes spatial awareness and hand–eye co-ordination. Deviation from this line increases perceptual distortion and makes operating more difficult. Changes in position of the surgeon or operating field during the operation should be accompanied by changing the position of the monitor/endoscopy tower. The use of a second (or third) monitor may improve surgical circumstances in specific procedures. An assistant should preferably hold the laparoscope while the surgeon uses both hands to control instrument manipulation, as would be the case in open surgery. The assistant should also be positioned in a more or less straight line with the monitor. The instrument cannulas should ideally be in a 30°–60° angle with the axis of the laparoscope port and surgical field, also referred to as ‘triangulation’ (Figs 24-1 and 24-8). If the angle is too small, instruments may obscure the operative site inside the abdomen and the accompanying short distance between the portals may reduce manipulation freedom of the instruments outside the abdomen. With a larger angle, depth perception is impaired and fine movements are more difficult.39,40 In order to create a comprehensive space for visualization, manipulation, and surgery, the abdominal cavity is insufflated with gas. Carbon dioxide is the preferred gas for the creation of pneumoperitoneum because it is inexpensive, highly soluble, chemically stable, rapidly eliminated, physically inert, suppresses combustion, and at physiological levels it is non-toxic. To further enhance access to certain tissues, the patient, lying in supine position, can be tilted into a head-down (Trendelenburg) or head-up (reverse Trendelenburg) position and towards a right or left lateral position, using gravity to move abdominal organs away from the area of interest. A motorized table that allows tilting is very useful for endoscopic surgery. In order to freely tilt the patient during surgery, the patient needs to be securely adhered to the table. Apart from tying the patient’s legs to the table, a moldable vacuum cushion greatly improves positioning (Fig. 24-2). Because of the obvious advantage of the small size of cats, positioning is relatively easy and repositioning during surgical procedures is possible if necessary. The need to move the animal should not impede the need to keep the procedure aseptic. Figure 24-2 Motorized surgery table showing Trendelenburg position and lateral tilt. On top are two moldable vacuum cushions and a heating pad. In the presence of CO2 pneumoperitoneum, transperitoneal absorption will cause an increase in partial arterial CO2 pressure (PaCO2), which may require mechanical ventilation to increase ventilation minute volume to facilitate expulsion of CO2. The most important event during laparoscopy that may negatively affect cardiovascular and respiratory function is the increase in intra-abdominal pressure (IAP) caused by pneumoperitoneum. Abdominal insufflation causes pressure on the diaphragm and abdominal blood vessels, resulting in a pressure-dependent increase in intrathoracic pressure, pulmonary vascular resistance, and systemic vascular resistance; and a pressure-dependent decrease in venous return, portal-venous blood flow, and abdominal visceral blood flow. These events result in an increase in peak-inspiratory airway pressure, heart rate, mean arterial blood pressure, and pulmonary arterial blood pressure; and a decrease in pulmonary compliance, tidal volume, minute ventilation, cardiac output, hepatic arterial, and renal arterial blood flow.41 In dogs and humans, an IAP up to 12 mmHg causes minimal cardiovascular and respiratory changes and is considered safe for laparoscopy.42,43 Higher pressures (>14 mmHg) may cause significant changes and should be avoided if possible.41,43–48 In humans, an IAP of <12 mmHg, caused less postoperative pain and discomfort than an IAP of >12 mmHg.49 Furthermore, an increase in IAP is not linearly related to an increase in abdominal space.50 Therefore, the lowest IAP providing adequate surgical space should be used, avoiding any unnecessary hemodynamic alterations. In dogs, an IAP of 8–10 mmHg was sufficient for laparoscopic ovariectomy (lapOVE).51,52 Of the few available descriptions of laparoscopic procedures in cats, most authors used an IAP of 8–12 mmHg,26,30,33–35 or up to 15 mmHg,28 which is merely a result of extrapolation of the technique that is used in dogs. In cats, however, effects of increased IAP have never been investigated. Furthermore, cats have a much more flexible body wall and skin that allows the creation of sufficient laparoscopic surgical space at much lower IAPs compared to dogs. We have found that a reduction in IAP to around 4–6 mmHg is sufficient in cats.29 A higher IAP is not needed for most procedures and may cause significant detrimental effects in this species and put them at an increased risk for complications. A Trendelenburg position may also cause cardiovascular changes. Depending on the amount (angle) of tilting, an increase in intrathoracic pressure compromises pulmonary function and baroreceptor reflexes cause generalized vasodilation and reduced heart rate and cardiac output. The reverse Trendelenburg position triggers baroreceptor reflexes resulting in vasoconstriction, increased heart rate and arterial blood pressure. Cardiac output is decreased, probably because of a decreased venous return.41 However, a 10–15° head-up or -down tilt is usually sufficient, and it does not cause major physiological changes, and the cardiovascular and respiratory effects of increased IAP generally dominate the situation.53,54 Because of the expected alterations in hemodynamic and respiratory function, cats should be carefully monitored during the application of pneumoperitoneum. Increased PaCO2 and intrathoracic pressure require increased ventilatory support, anticipating higher ventilation pressures and reduced lung volume, and aiming for normocapnia. Mechanical intermittent positive pressure ventilation (IPPV) should be considered. Positive end expiratory pressure ventilation (PEEP) should not be used because it further increases intrathoracic pressure, depressing cardiopulmonary function.55,56 One should be aware that in unstable cardiovascular or pulmonary patients, the effects of increased IAP and tilting of the body can be more severe and even dangerous. Furthermore, general anesthesia aggravates the effects of increased IAP and tilting and one could consider a combination of sedation and local anesthesia for laparoscopic procedures in critical patients.57 The use of local anesthetic infiltration of portal sites using lidocaine, bupivicaine or chirocaine has been shown to significantly improve postoperative analgesia in humans.58 However, a significant advantage of bupivacaine infiltration of portal sites was not found in a recent controlled clinical trial in dogs.59 A Trendelenburg position may reduce the chance for splenic trauma, because the spleen tends to slide craniolaterally away from the insertion point.28,60 Proper placement of the Veress needle into the abdominal cavity can be checked by the ‘hanging drop’ test. Using this test, a drop of sterile saline solution is applied to the hub of the needle and should be sucked into the abdomen by the negative IAP. The test is not fail-safe due to occlusion of the tip of the needle from contact with an organ or omentum. Possible occlusion can be judged by first flushing the Veress needle with 1–2 mL of sterile saline or lifting up the abdominal wall to move the tip away from any organ and then repeating the hanging drop test.28,60 The use of a low IAP, which is preferred in cats, may limit the possibilities for primary trocar insertion because the abdominal wall is under relatively low tension and will move inwards with pressure exerted on it when trying to puncture it with a trocar, increasing the chance for iatrogenic damage. Some authors overcome this difficulty by using a higher IAP for initial port placement, after which IAP is set to a lower value.9,52 However, trocar insertion can be facilitated using stay sutures to stabilize the abdominal wall during insertion or by using threaded cannulas that can be screwed through a small stab incision in skin and fascia. Abdominal wall-lifting techniques have been described for direct primary trocar insertion in cats.29 We prefer to perform direct trocar insertion using a semi-open technique: first a small skin incision is made (about the diameter of the trocar to be inserted) and the subcutaneous tissue bluntly dissected to reveal the linea alba. The linea alba is carefully lifted with forceps, and stay sutures placed at both corners (cranial and caudal) of the incision. To ensure enough strength, the stay sutures pass through both skin and linea alba. A 2–3 mm incision is made through the abdominal wall at the linea alba. This incision is kept smaller than the cannula diameter to provide a good tight fit of the cannula. Incising the abdominal wall facilitates entry of air, which together with lifting the abdominal wall, should prevent abdominal organs from being lifted with the abdominal wall which could occur due to negative pressure-adherence with the closed approach. The abdominal wall is lifted up while the trocar is inserted (Fig. 24-3). Using a blunt trocar or threaded cannula is the safest entry technique. Figure 24-3 Abdominal entry. (A) The linea alba is grabbed and lifted up while (B) stay sutures are placed in the cranial and caudal border of the skin incision, penetrating skin, subcutaneous tissue, and linea alba/external rectus fascia. (C) The stay sutures are used to pull up the abdominal wall while inserting the trocar. After trocar placement, the stay sutures can be used to fixate the cannula. (D,E) Stay sutures can also be used for insertion of secondary trocars, which are placed under laparoscopic guidance (F). The placement of a second or more trocars is then safely performed under laparoscopic guidance (Fig. 24-3). Transillumination from within the abdomen helps to avoid puncturing blood vessels in the abdominal wall during trocar insertion. This is very easy and useful in cats because of their thin abdominal wall. If the low IAP complicates proper entry of a sharp trocar, stay sutures may be used to stabilize the abdominal wall during trocar insertion (Fig. 24-3). In order to reduce the number of cannulas needed for a specific procedure, transabdominal suspension sutures may be used to keep tissues lifted up for surgical access without using extra laparoscopic forceps.61 This creates a fixed position of the tissues and decreases freedom of manipulation. The flexible abdominal wall of cats facilitates ‘lifting up’ procedures, but care needs to be taken not to apply too much tension, which could result in the stay suture being pulled out of the tissue. An alternative to pneumoperitoneum has been evaluated in five cats using a custom-made abdominal wall-lifting device to pull the abdominal midline upwards to create a surgical space for laparoscopy without using gas insufflation. However, this technique seemed to be associated with poorer visualization of the abdominal cavity compared to pneumoperitoneum, necessitating conversion to laparotomy in one cat. In particular, lateral intra-abdominal space was reduced because of the upward ‘tenting’ effect of abdominal wall lifting compared to the dome-shape of pneumoperitoneum.62 The rigid optical laparoscope preferably is composed of a Hopkins rod lens system, which has a relatively wide field of view and bright image. A laparoscope with 0° or 30° viewing angle is adequate for most laparoscopic procedures. The 30° viewing angle allows observation of abdominal organs from different angles by rotating the telescope. The diameter of the scope determines the maximum width of the field of view and the amount of light passing through. For cats we recommend a 2.7–5 mm diameter endoscope for laparoscopic and thoracoscopic procedures (Fig. 24-4). In our opinion, the advantage of a further decrease in size does not compensate for the smaller and less bright field of view. We commonly use a 3.9 mm diameter laparoscope (Hopkins II, Storz) with 4.5 mm diameter cannula because of its superb image quality compared to smaller diameter scopes. Furthermore, smaller scopes are usually used with a protective sheath, increasing the total diameter without enhancing the image. The endoscope is connected to a camera system with monitor. Camera resolutions range from single CCD-chip (450 horizontal lines, poor color reproduction) to three CCD-chips (750 horizontal lines and good color quality) to full HD (1080 horizontal lines and 16 : 9 widescreen image; Fig. 24-5). The most popular light sources use xenon lamps, being much brighter and whiter than halogen.7,9,63 It can be helpful to be able to capture images and video clips of your laparoscopic procedures. Although dedicated devices are on the market, digital recording devices can be bought relatively inexpensively nowadays and several laptop computers enable digital video capturing as a standard feature. Figure 24-4 Endoscopic surgery instruments. (A) Basic pediatric instrument set with 3 mm diameter instruments, a 3.9 mm diameter laparoscope (Hopkins II, Storz), 3.8 mm and 4.5 mm outer diameter trocars. (B) Ternamian EndoTip threaded cannula (Storz). (C) Biopsy cup forceps, straight grasping forceps, curved Kelly forceps, and scissors; (D) two types of bipolar forceps; (E) HD camera (Storz). A basic set of instruments for laparoscopic surgery contains grasping forceps (Kelly, Babcock, etc), a biopsy forceps, a palpation probe, scissors, and bipolar forceps or other vessel-sealing device (Fig. 24-4). For cats we recommend the use of 3 mm pediatric instruments.64 A suction/irrigation device can be helpful to maintain visualization of tissue structures in case of hemorrhage, which can dramatically obscure the surgical field. Because the smallest vessel-sealing devices are 5 mm in diameter, port size needs to be sacrificed for ease and speed of surgery in certain cats. A trocar is the combination of a cannula (or sleeve) and obturator. Cannulas function as instrument portals in the abdominal wall. Placement through the abdominal wall can be facilitated by the use of a sharp obturator. Puncturing the abdominal wall with a sharp trocar has the advantage of creating a tight fit between cannula and body wall. A disadvantage is the risk of damaging an organ iatrogenically during blind entry (i.e., placement of primary trocar). A safer entry may be facilitated by using a blunt threaded cannula without an obturator, which has the benefit of also resulting in a tight fit.65 A blunt trocar can be used with an open entry technique. A cannula for laparoscopy contains an automatic valve to prevent leakage of CO2 gas when no instrument is inserted and a rubber washer to prevent gas leakage between instrument and cannula. A cannula with a Luer lock valve can be used for insufflation of the abdomen and instillation of fluids. Cats have a thin and flexible skin and abdominal wall. Smaller and lighter cannulas reduce surgical trauma (incision length) and reduce problems such as cannulas slipping in and out of the abdomen and the weight of the cannula pushing onto the abdominal wall, reducing surgical space. Because of the small size of cats, smaller-sized instruments greatly improve surgical performance. Figure 24-4A displays a basic pediatric instrument set that may be used for endoscopic surgery in cats, containing 3 mm diameter laparoscopic equipment with 3.8 mm outer diameter cannulas. Specially designed reusable cannulas containing silicone leaflet valves and plastic casing further reduce weight. Because of the abdominal wall anatomy of cats, slipping of cannulas in and out of the abdominal wall incisions can pose a problem.28,29 To avoid this, it is important to make the initial portal incisions smaller than the cannula size, which can be challenging when using an open entry technique. The use of threaded cannulas (Ternamian EndoTip, Storz, Fig. 24-4B) or Hasson trocars that can be sutured to skin can improve cannula stability in the abdominal wall. Threaded cannulas also have the advantage of not needing a sharp obturator to facilitate placement through the abdominal wall. Instead, the cannula is ‘screwed’ in place through a small incision, which can be visualized by inserting a 0° laparoscope.65 Threaded cannulas are also available in pediatric sizes (3.9 mm inner diameter; see also Chapter 42). Another option is the use of a purse-string suture around the incision to tighten the cannula in the abdominal wall. When stay sutures are used for primary trocar entry, they can be wound around the cannula and secured with mosquito forceps to add stability (Fig. 24-3). Surgeons that perform arthroscopy can use some of the available 2.7 mm equipment on cats. The size and length of the equipment is of course also an important consideration.
Endoscopic surgery in cats
Laparoscopy
Laparascopic surgery in cats
Basic surgical principles
Pneumoperitoneum, patient positioning, and anesthetic considerations
Abdominal access

Equipment
Optical and video set-up




Standard instruments
Trocars/cannulas
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Veterian Key
Fastest Veterinary Medicine Insight Engine


