3 Emergency database interpretation
Packed cell Volume and Plasma Total Solids
Manual PCV and TS should always be interpreted together and the changes identified will raise the index of suspicion for particular causes (see Table 3.1).
Table 3.1 Interpretation of manual packed cell volume and plasma total solids
| Packed cell volume (%) | Plasma total solids (g/L) | Causes to consider |
|---|---|---|
| Decreased | Normal | |
| Decreased | Decreased | |
| Normal | Increased | |
| Normal | Decreased | |
| Increased | Normal | |
| Increased | Increased | Dehydration |
When interpreting changes in all laboratory parameters, including PCV and TS, it is important to remember that normal ranges cited for adult dogs and cats may not be applicable to puppies and kittens (see Ch. 41).
Gross Plasma Appearance
Common abnormalities of plasma appearance and possible causes are listed in Table 3.2. In addition to plasma appearance, samples can be evaluated for the size of the buffy coat following centrifugation, with a large buffy coat suggestive of leukocytosis.
Table 3.2 Possible causes of abnormalities in gross plasma appearance
| Plasma appearance | Possible causes |
|---|---|
| Haemolysed | |
| Icteric | |
| Lipaemic |
Azotaemia
The causes of azotaemia may be divided into prerenal, renal or postrenal.
Renal azotaemia
Clinical Tip
Peripheral Blood Smear Examination
Peripheral blood smear examination is recommended for the majority of emergency patients. Cytology allows cell morphology to be evaluated and abnormal cell populations to be identified; a degree of quantitative information can also be obtained. Red blood cells, white blood cells and platelets are evaluated (Figures 3.1 and 3.2).
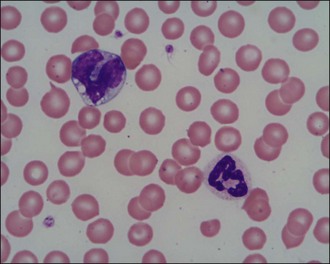
Figure 3.1 Normal canine red blood cells, neutrophil, monocyte and platelets (×1000)
(Photograph courtesy of Kate English).
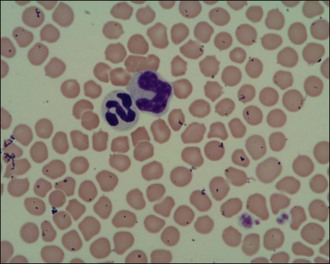
Figure 3.2 Normal feline red blood cells, neutrophil, monocyte and platelets (×1000)
(Photograph courtesy of Kate English).
Red blood cells
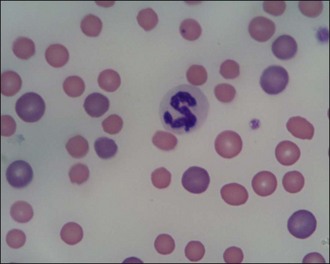
Red blood cells are examined for variability in size (anisocytosis) and colour (polychromasia) (Figure 3.3), both of which are suggestive of regenerative anaemia. When stained using a Romanowsky stain such as Diff-Quik, immature red blood cells (polychromatophils), which are larger than mature cells, have a purplish- or bluish-tinged appearance.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


