E
Echinococcosis
BASIC INFORMATION
DEFINITION
EPIDEMIOLOGY
SPECIES, AGE, SEX
RISK FACTORS
Exposure and ingestion of intermediate hosts (rodents, cattle, sheep) harboring the hydatid cysts
CONTAGION & ZOONOSIS
CLINICAL PRESENTATION
HISTORY, CHIEF COMPLAINT
ETIOLOGY AND PATHOPHYSIOLOGY
DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
Other taeniids, to include many tapeworms within the genera Taenia and Multiceps.
TREATMENT
TREATMENT
PEARLS & CONSIDERATIONS
PREVENTION
Eckert J, Thompson RC, Bucklar H, Bilger B, Deplazes P. Efficacy evaluation of epsiprantel (Cestex) against Echinococcus multilocularis in dogs and cats. Berl Munc Tierarztl Wochenchr. 2001;114(3–4):121-126.
Jenkins DJ, Romig T. Milbemycin oxime in a new formulation, combined with praziquantel, does not reduce the efficacy of praziquantel against E. multilocularis in cats. J Helminthol. 2003;77(4):367-370.
Eclampsia ![]()
BASIC INFORMATION 
EPIDEMIOLOGY
GENETICS & BREED PREDISPOSITION
More likely to occur in small-breed dogs, although any lactating bitch may be affected
CLINICAL PRESENTATION
HISTORY, CHIEF COMPLAINT
Lactating bitch with signs of aberrant behavior, ataxia, muscle tremors, seizures, and/or tetany
TREATMENT 
ACUTE GENERAL TREATMENT
CHRONIC TREATMENT
NUTRITION/DIET
PROGNOSIS AND OUTCOME 
Prognosis is good to excellent with immediate treatment and subsequent management.
PEARLS & CONSIDERATIONS 
COMMENTS
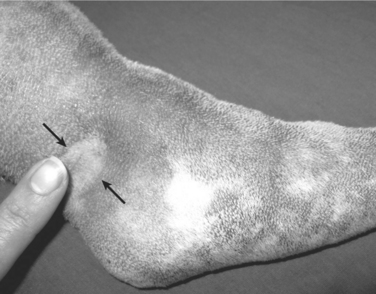
Edema, Subcutaneous
BASIC INFORMATION 
SYNONYMS
Peripheral edema (edema of the paws and legs), anasarca (generalized, massive subcutaneous edema)
CLINICAL PRESENTATION
HISTORY, CHIEF COMPLAINT
Limb swelling or a swollen appearance may be historical findings suggestive of subcutaneous edema.
PHYSICAL EXAM FINDINGS
TREATMENT 
ACUTE AND CHRONIC TREATMENT
PROGNOSIS AND OUTCOME 
The prognosis for patients with subcutaneous edema depends on the underlying condition and the ability to treat and resolve this primary disease. Edema due to inflammation or infection, congestive heart failure, or hypoproteinemia can often be successfully managed or resolved. Treatment response for lymphatic obstruction is variable; lymph-edema (see p. 667) can be challenging to manage long term, and there is no curative therapy.
Mathews KA. Monitoring fluid therapy and complications of fluid therapy. In: Dibartola SP, editor. Fluid, electrolyte, and acid-base disorders in small animal practice. ed 3. St Louis: Elsevier Saunders; 2006:385.
Raffe MR, Roberts J. Edema. In: Ettinger SJ, Feldman EC, editors. Veterinary internal medicine. ed 6. St Louis: Elsevier Saunders; 2005:70.
Ehrlichiosis, Canine Monocytic
BASIC INFORMATION 
EPIDEMIOLOGY
GENETICS & BREED PREDISPOSITION
German shepherd dogs have a more fulminant illness, owing to reduced cellular immune response.
CLINICAL PRESENTATION
DISEASE FORMS/SUBTYPES
HISTORY, CHIEF COMPLAINT
PHYSICAL EXAM FINDINGS
ETIOLOGY AND PATHOPHYSIOLOGY
DIAGNOSIS 
INITIAL DATABASE
ADVANCED OR CONFIRMATORY TESTING
TREATMENT 
TREATMENT OVERVIEW
ACUTE GENERAL TREATMENT
DRUG INTERACTIONS
PROGNOSIS AND OUTCOME 
PEARLS & CONSIDERATIONS 
COMMENTS
Eisenmenger’s Syndrome
BASIC INFORMATION
SYNONYMS
EPIDEMIOLOGY
GENETICS & BREED PREDISPOSITION
Dependent on the underlying cause:
ETIOLOGY AND PATHOPHYSIOLOGY
DIAGNOSIS
INITIAL DATABASE
TREATMENT
ACUTE GENERAL TREATMENT
CHRONIC TREATMENT
BEHAVIOR/EXERCISE
Restrict exercise and excitement in patients with collapsing or syncopal episodes.
PROGNOSIS AND OUTCOME
Long-term prognosis is guarded to poor, depending on severity of pulmonary hypertension.



