E
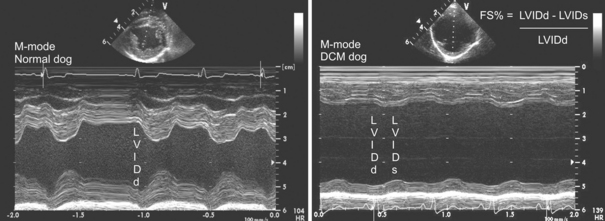
Echocardiography
INDICATIONS
EQUIPMENT, ANESTHESIA
PREPARATION: IMPORTANT CHECKPOINTS
POSSIBLE COMPLICATIONS AND COMMON ERRORS TO AVOID
PROCEDURE
Bonagura JD. Echocardiography. J Am Vet Med Assoc. 1994;204:516-522.
Oyama MA. Advances in echocardiography. Vet Clin North Am Small Anim Pract. 2001;34(5):1083-1104.
Thomas WP, Gaber CE, Jacobs GJ, et al. Recommendations for standards in transthoracic two-dimensional echocardiography in the dog and cat. J Vet Intern Med. 1993;7:247-252.
Electrocardiography
EQUIPMENT, ANESTHESIA
POSSIBLE COMPLICATIONS AND COMMON ERRORS TO AVOID
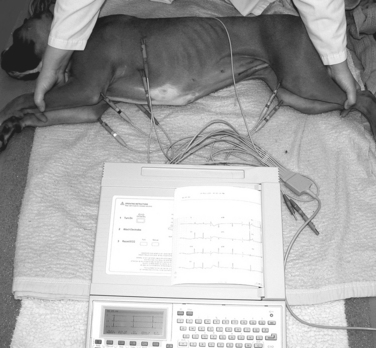
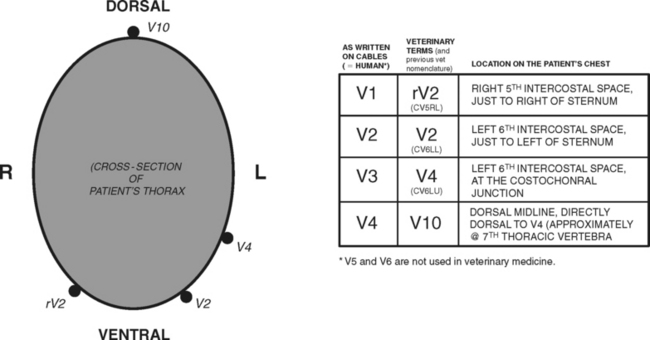
ECG Clip/Electrode Placement for Standard Limb Leads (I, II, III, aVR, aVL, aVF)
| RA, white | Right forelimb; clip to skin just proximal to the olecranon (caudal triceps region). |
| LA, black | Left forelimb; clip to skin just proximal to the olecranon (caudal triceps region). |
| RL, green | Right hind limb; clip to skin just proximal to the stifle (cranial thigh); ground wire. |
| LL, red | Left hind limb; clip to skin just proximal to the stifle (cranial thigh). |
PROCEDURE
POSTPROCEDURE
The clips are carefully detached from the skin prior to releasing the animal’s restraint.
ALTERNATIVES AND THEIR RELATIVE MERITS
Electromyography (EMG) and Motor Nerve Conduction Velocity (NCV)
OVERVIEW AND GOALS
INDICATIONS
EQUIPMENT, ANESTHESIA
PREPARATION: IMPORTANT CHECKPOINTS
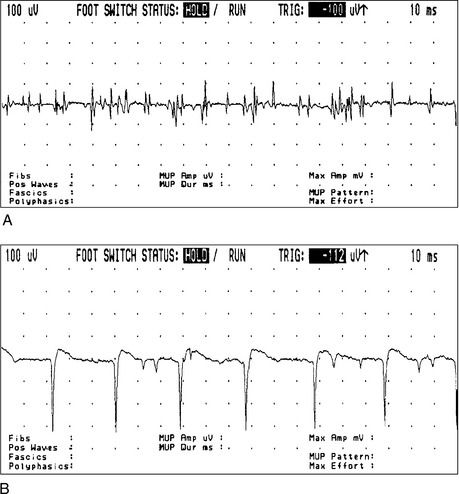
PROCEDURE
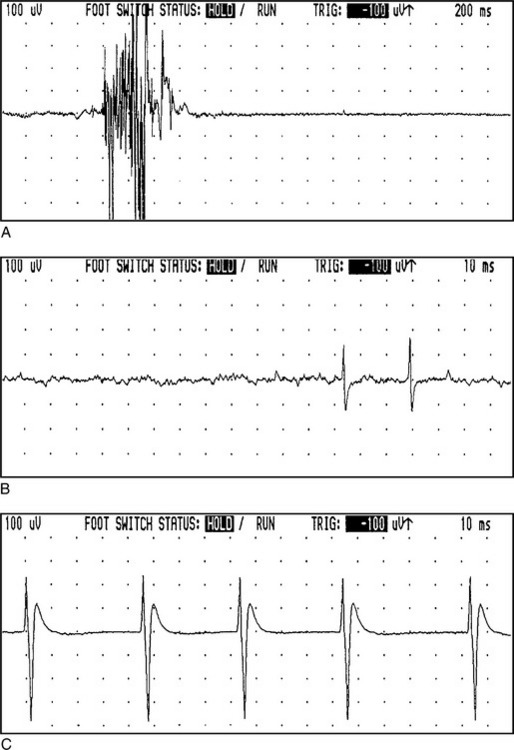
(Reprinted with permission from Cuddon PA: Electrophysiology in neuromuscular disease, Vet Clin North Am Small Anim Pract 32:31-62, 2002.)
(Reprinted with permission from Cuddon PA: Electrophysiology in neuromuscular disease, Vet Clin North Am Small Anim Pract 32:31-62, 2002.)
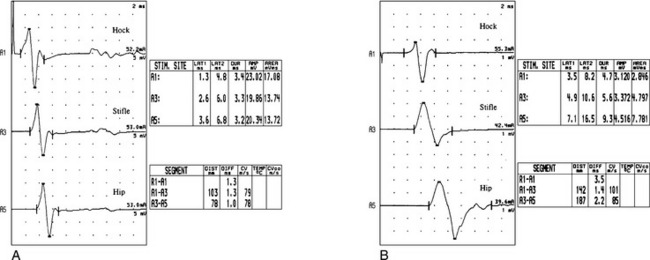
(Reprinted with permission from Cuddon PA: Electrophysiology in neuromuscular disease, Vet Clin North Am Small Anim Pract 32:31-62, 2002.)



