Chapter 67 Digital Radiography of the Elephant Foot
Foot disease is a major cause of captive elephant morbidity and mortality.4,6,10 Common foot problems encountered at the nail, skin, sole, or pad include penetrating injuries, trauma, cracks in the sole, nail, or cuticle, overgrown nail, sole, or cuticle, laminitis, ingrown nails, pododermatitis, osteomyelitis, arthritis, fractures, dislocations, abscesses, and degenerative joint disease.2,5,12,13 Chronic foot disease that is unresponsive to medical and/or surgical management ultimately results in euthanasia.9,17 Annual examination of captive elephants are recommended by the North American Species Survival Plan (SSP), including foot radiography in elephants with chronic foot disease.14
To date, elephant foot radiography reports have focused on conventional analog radiography (AR) techniques.7,8,14 Recent advances in diagnostic medical imaging include the use of digital radiography (DR) for the clinical assessment of foot pathology in the captive elephant.
Digital Radiography Overview
Conventional radiography produces images using film coated with a light-sensitive, silver halide–containing emulsion. After exposure to x-rays or light, the silver halide crystals precipitate and remain on the film during processing. The amount of precipitation is directly related to processed film blackness. Film speed corresponds to the size or amount of silver halide crystals. High-speed films have crystals that are larger or more numerous. X-rays are more likely to precipitate these crystals, which will cause a greater area of exposure than with a slower speed film, resulting in less image detail with high-speed films. Intensifying screens in the form of film cassettes are used to convert x-rays to visible light to expose the film, because the film emulsion is more sensitive to light.16 Using conventional analog techniques, standard portable radiographic units with 80 to100 kVp and 15 mA have produced reliable, diagnostic elephant foot radiographs.7,14
CR uses a detector, or image plate (IP), for image acquisition, an IP reader, an analog-to-digital converter (ADC), and a computer and software programs to process the digital image.1,18 The IP is similar in appearance to conventional cassettes and is not directly attached to a computer. The IP functions similarly to conventional film-screen combinations, but uses photosensitive phosphors for image capture rather than crystals. The phosphors allow for latent image capture following x-ray exposure, similar to latent image capture with analog systems. In contrast to conventional radiography, CR latent images decay rapidly (minutes to days) and must be processed rapidly. The CR reader processes the latent image by converting stored energy into visible light and then into analog electrical signals, which are passed through an ADC to create a digital image for display on a computer monitor. Finally, the IP is erased using high-intensity white light to release residual energy, making the IP available for immediate reuse. The IP may be reused multiple times, with the actual number varying with protective plate quality and care during processing.
Computer software is used to process the digital image. Image contrast enhancement is possible with all digital imaging software using look-up tables (LUTs). LUTs enhance contrast by increasing the difference among anatomic structures using preset pixel values specific for different body systems (e.g., thorax, abdomen, musculoskeletal). Default software settings also determine edge enhancement (sharpness), contrast resolution, and brightness.18 Manual manipulations to adjust factors such as contrast, brightness, sharpness, and size can also be carried out.
In contrast to CR, DDR uses an integrated readout mechanism within the IP, producing a digital image following x-ray exposure that is sent directly to a computer via an attached cable.1,18 Image acquisition is faster with DDR, because the need for an image-plate reader is eliminated. The IPs used in DDR include flat panel detectors (FPDs) and charge-coupled devices (CCDs). Both direct-converting and indirect-converting FPDs are available to transform x-rays into electrical signals. The specifics of direct and indirect FPDs are beyond the scope of this chapter, but are available in the literature. Image capture involves transforming x-rays to visible light, then to electrical charges, and finally from analog-to-digital format during the readout process.16 The image minification process for visible light transformation into electrical signals with CCDs may result in greater image noise compared with FPDs. CCD systems also require more housing space than FPDs because of the optical system of the CCD and are nonportable, but tend to be less expensive than FPDs. Because of their nonportability, CCD systems are not currently applicable to large animal imaging outside the hospital setting. Comparisons among commercially available flat panel detectors are available. Digital data are processed on the computer as described for CR systems (see earlier).
Compared with DDR, CR’s main disadvantage is the lack of direct readout. This becomes significant for the evaluation of elephants and other large mammals in which health examinations are conducted on site and not in the hospital setting. Using DDR, diagnostic digital images are obtained, processed, and evaluated patient side, eliminating the need to transport plates to the hospital for processing and evaluation. In addition, DR uses a single IP multiple times during a radiographic assessment, whereas CR uses multiple IPs that must be erased by the reader before reuse. Despite these limitations, CR is a more mature technology that has benefited from improvements and advancements over the years, whereas DDR is a relatively young imaging system.18 In addition, with CR systems, the plate is not connected to a computer by a wire, an advantage when working with large animals. Both digital imaging systems enable users to send image data to a picture archiving communications system (PACS) for analysis and storage. We expect to see continued advancement for both technologies in the future as digital radiography becomes more available to zoological and wildlife veterinarians.
Analog Versus Digital
Image format is the largest difference between the two systems. With AR, once the radiograph is printed, image adjustment is not possible. For digital radiographs, many factors may be manipulated following image acquisition that affect image appearance; these include contrast, brightness, magnification, monitor luminance, monitor size, and display resolution.16,18,19 In addition to image format, digital systems allow for more rapid results given the ability to reuse cassettes without a need for replacing film (CR) or direct read-out ability (DDR). In this respect, DDR is especially beneficial because radiographs are available in seconds patient side, with fewer retakes necessary, allowing for rapid technique adjustments, modification of patient positioning, and radiographic assessments to obtain diagnostic images. The decreased time delay with digital systems becomes increasingly important when radiographing all digits on the four limbs at annual or baseline elephant foot examinations. Although digital systems lack the degree of spatial resolution possible with film-screen combinations, both digital radiography systems have diagnostic image quality equal to or better than that of analog radiology. This is largely because of superior contrast resolution and processing functions available with digital systems.1
Conventional radiography is further limited by the narrow exposure range, need for darkroom quality control, processor and chemical maintenance, cost of upkeep and purchase of chemicals and film, and hard copy image storage.18 In contrast, digital radiography eliminates the need for film and chemicals, decreases the number of exposures for diagnostic images, decreases technician workload, and allows for rapid image acquisition.1 Digital images are stored electronically—although some practices still prefer to maintain both hard and soft copies of patient records—and allow for easy remote consultation with specialists via the electronic exchange of digital images. Image capture, display, storage, adjustment, and communication are available for digital systems using PACSs.1 In addition, digital imaging communications in medicine (DICOM) image file formats may be used for manipulation and storage of digital images from various medical imaging devices such as DR systems, as well as others such as computed tomography, magnetic resonance imaging, and ultrasound. DICOM allows for connectivity with PACS regardless of imaging modality or specific product used. Upkeep of digital systems may involve PACS software maintenance and general equipment and software upgrades, as well as monitor calibrations to minimize electronic image fading.19
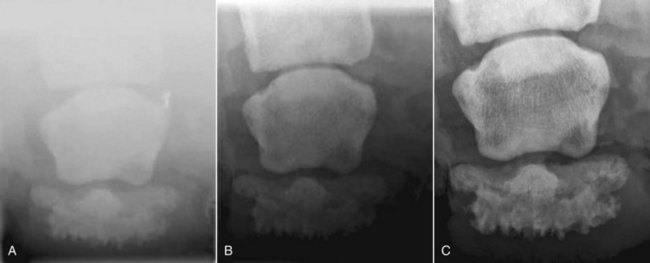
Both CR and DDR offer improved exposure latitude, image contrast, and postimage capture processing ability compared with conventional radiography.3,7 However, all three modalities require similar power techniques.1 Because DR systems have a linear response to x-ray exposure (compared with a sigmoid response with conventional radiography), there is a wider exposure operating range, allowing for viewing of soft tissues and bony structures on the same image using the same exposure and technique. This becomes important in elephant foot radiography when assessing disease states of the soft tissues of the foot (e.g., cuticle, nail) and how they relate to the underlying bony structures (phalanges). Figure 67-1 displays D3 P3 from the same elephant using AR, CR, and DDR radiographic techniques.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


