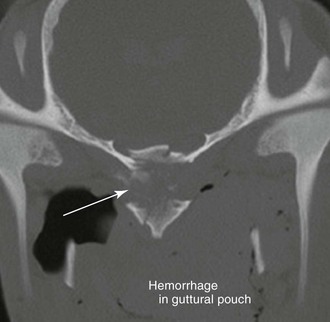
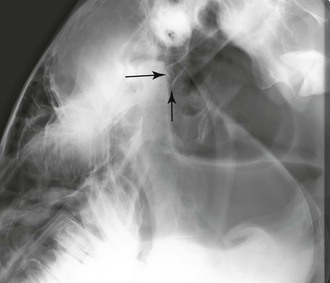
Charlotte Sinclair, Anthony P. Pease In young horses, the basisphenoid-basioccipital bone that constitutes the ventral aspect of the cranium has an open suture between the basisphenoid bone and basioccipital bone (Figure 95-1). This suture is the last to close radiographically and does so when the horse is about 5 years of age. In young horses, this suture can radiographically mimic a fracture. For this reason, when a horse is being evaluated for traumatic injury involving the ventral aspect of the cranium, it is important to search for bone displacement at the site of the fracture and to evaluate the guttural pouches (Figure 95-2). In the latter, hemorrhage, wall hematoma, and compression of the lateral compartment are important radiographic signs of trauma to the basisphenoid and basioccipital bones. The longus capitis muscle (rectus capitis ventralis major) originates on the transverse processes of cervical vertebrae C3 and C5 and inserts on the tubercles at the junction of the basilar part of the occipital bone with the body of the basisphenoid bone; this muscle flexes the head dorsoventrally and laterally. The rectus capitis ventralis (rectus capitis ventralis minor) is a smaller muscle that lies dorsal to the longus capitis (LC). It originates from the ventral arch of the atlas and inserts on the basioccipital bone (close to the insertion of LC), and it functions to flex the atlanto-occipital joint. The rectus capitis ventralis (RCV) and LC muscles can be seen within the medial margin of the medial compartment of the guttural pouch. The digastricus muscle is evident beneath the mucosa in the lateral compartment of the guttural pouch; it originates at the jugular process of the occipital bone and inserts onto the medial surface of the ventral border of the mandible. Traumatic injury involving the ventral cranium most often occurs in horses with a history of rearing and falling over backward or in which the head became entrapped in a gate or fence. Overextension of the atlanto-occipital joint caused by the external occipital protuberance acting as a fulcrum can result in rupture of the LC, RCV, or both, causing disruption of the guttural pouch and associated hemorrhage either alone or in conjunction with an avulsion fracture of the basisphenoid-basioccipital bone (Figures 95-3 and 95-4). This avulsion and fracture of the basisphenoid and basioccipital bones generally happens in horses younger than 5 years, when the physis is still open. In older horses, generally the muscle will avulse without the bone fracturing. If a ventral skull fracture is present, the horse is likely to have concurrent neurologic signs, whereas in cases of head flexor muscle rupture alone, neurologic deficits are rare.
Diagnosis of Ventral Cranial Trauma
Anatomic Overview of the Ventral Cranium
Etiology and Presenting Signs of Ventral Cranial Trauma
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Diagnosis of Ventral Cranial Trauma
Chapter 95

Only gold members can continue reading. Log In or Register to continue
