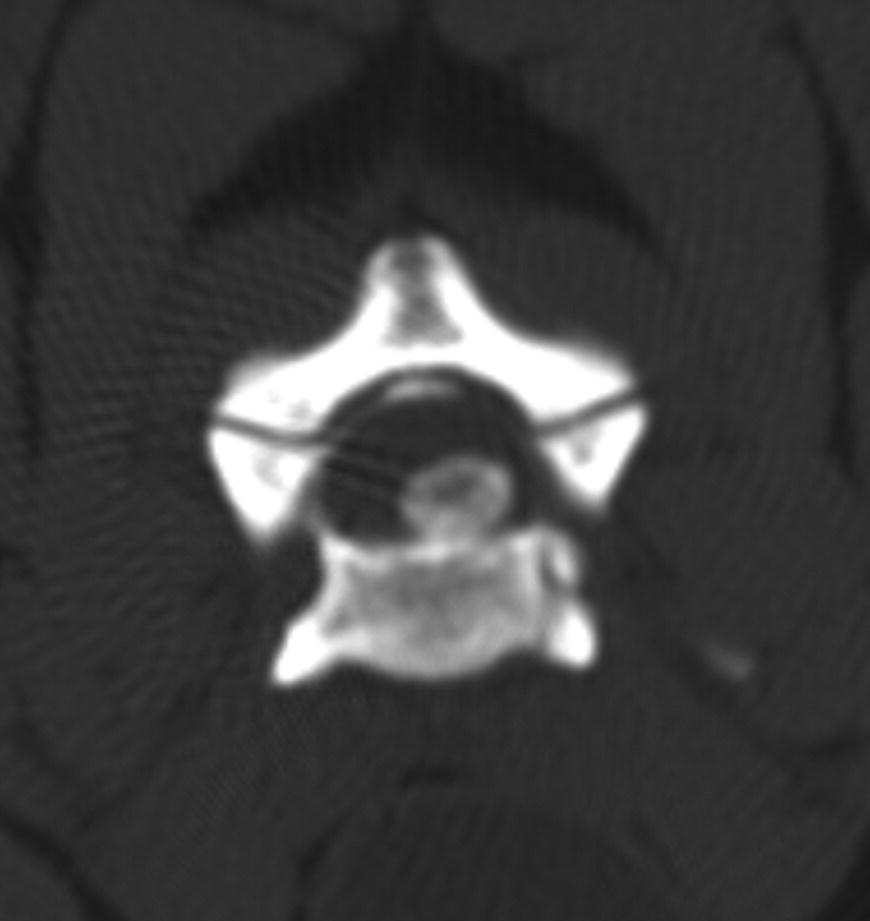
30 Amy E. Fauber Once a patient with a cervical intervertebral disc herniation has been deemed a surgical candidate, the surgeon is faced with several options on how to operate. A general rule of thumb is to establish a goal of mass (disc) removal, as this is ultimately the decompressive element of surgery. A challenging decision comes when the herniated disc material is lateralized and residual material may remain in the intervertebral foramen without a carefully planned and executed approach. In these instances, it is not always clear which approach will best allow for spinal cord and nerve root decompression. Also challenging is the current lack of biomechanical studies comparing the instability created by these different approaches or the clinical significance of any such instability. The ventral slot is one of the most widely used approaches for spinal cord decompression in veterinary patients with cervical intervertebral disc herniation. Using this procedure, it is very easy to access displaced disc material located within the ventral aspect of the vertebral canal (see Figure 30.1). This procedure was first described in dogs as an alternative to the dorsal approach for laminectomy or hemilaminectomy [1]. Either a ventral midline dissection or a paramedian dissection to the ventral cervical spine can be used. For the midline approach, a ventral midline incision is made and the approach is continued on the midline between the paired sternothyroideus and sternohyoideus muscles. The trachea, carotid sheath, and esophagus are retracted to the left to expose the paired longus colli muscles immediately ventral to the vertebrae [2]. For the paramedian approach, a ventral midline skin incision is made, but the dissection is continued paramedian, between the right sternocephalicus muscle and right sternothyroideus muscle [3]. The sternohyoideus and sternothyroideus muscles, trachea, esophagus, and carotid sheath are all retracted to the left. The paramedian approach may make it less likely to disrupt tracheal blood supply, the right carotid sheath, and the recurrent laryngeal nerve [3]. With either of these ventral approaches, the correct site for the ventral slot is identified by palpating the large transverse processes of C6 and the ventral midline process of C1 and then, using these landmarks, palpating the caudal ventral processes of the cervical vertebrae that mark each interspace between C2–C3 and C7–T1. It is important to review preoperative imaging to identify any anatomical variations in vertebral formula or transitional vertebrae. The longus colli muscle is divided along the midline to expose the ventral aspects of the vertebral bodies and intervertebral disc. A high-speed burr is used to create an opening (“slot”) in the vertebral bodies, centered over the disc space and extending to the dorsal longitudinal ligament. Due to the angulation of the intervertebral disc and end plates, the slot should be centered initially over the caudal aspect of the cranial vertebra rather than over the ventral annulus, with the caudal extent of the slot at the cranial end plate of the caudal vertebra. As the burring is continued dorsally, the slot will end up being centered on the dorsal aspect of the intervertebral disc. This will help avoid disruption of the paired vertebral venous plexus, which deviates laterally over each disc space, and thus reduce the risk for hemorrhage, which can be quite severe and interfere with completion of the disc removal and decompression. After penetrating the dorsal cortex of the vertebral body, the dorsal longitudinal ligament is separated or excised, and the herniated disc material is removed from the vertebral canal using instruments such as a right-angle nerve root retractor passed gently along the ventral aspect of the vertebral canal. Figure 30.1 Transverse CT image at the level of C4–C5 demonstrating a ventral disc extrusion. Complications of the ventral slot include hemorrhage from the vertebral venous plexus, instability of the vertebral bodies, erosion of the dorsal tracheal membrane from sutures in the longus colli, and poor decompression due to the limited visibility through the slot created [1, 4–7]. The reason the ventral approach is confined to a slot, and not a larger window that would permit more visualization and room for manipulation of instruments, is because of the potential for vertebral collapse and fracture from an overly aggressive degree of bone removal from the vertebral bodies. This is less a problem in human anterior approaches owing to the short but wide morphology of cervical vertebrae in that species, compared with the long but narrow cervical vertebrae in dogs. The small size of the resultant windows created in dogs, along with the small overall size of many veterinary patients, means that there is very little working room for either visualization or manipulation of instruments in our patients. So while the ventral approach provides the most direct route to ventrally herniated disc material, and without the degree of dissection required for dorsal approaches, it comes with the trade-off of very limited working space. The use of magnification and good lighting can mitigate some of these inherent limitations, but this remains one of the limiting aspects to this approach in dogs. A dorsal approach to the cervical spine has been described and used for decompression of ventral disc displacements if there is a combined ventral disc displacement and dorsal compression (see Figure 30.2
Cervical Disc Disease: Ventral Slot versus Hemilaminectomy versus Dorsal Laminectomy
Introduction
Ventral approach and ventral slot
Dorsal approach and dorsal laminectomy
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


