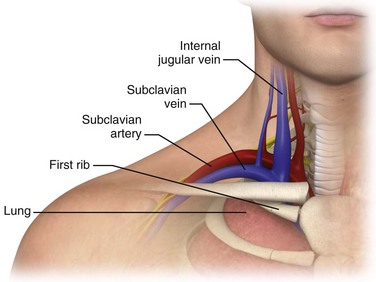
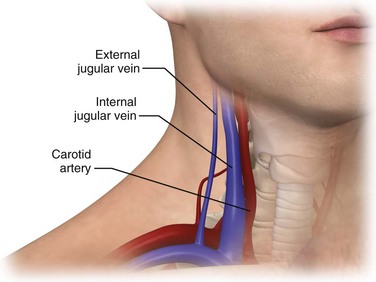
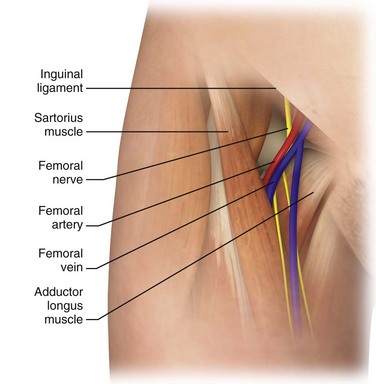
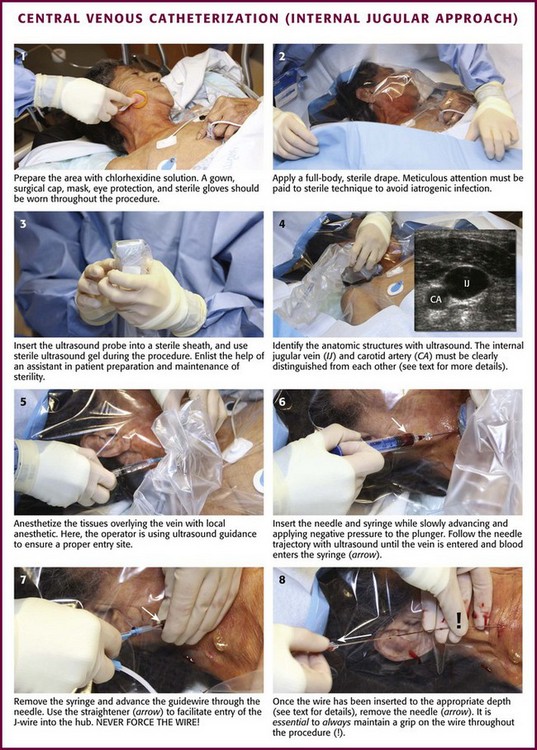
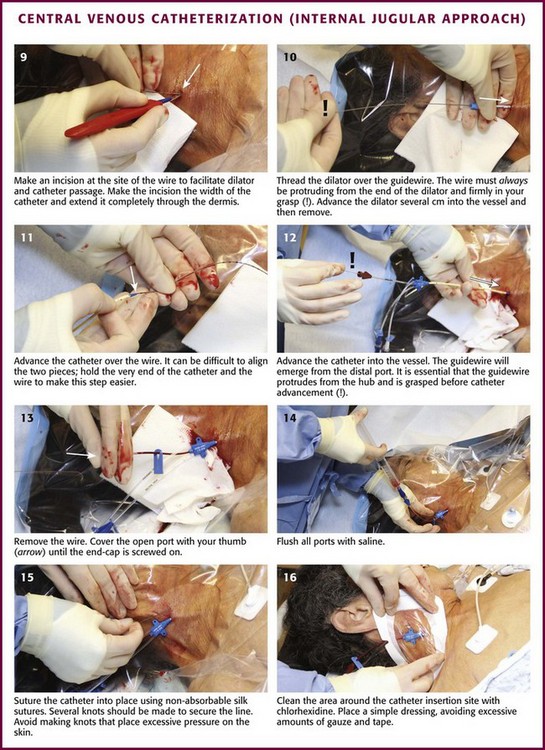
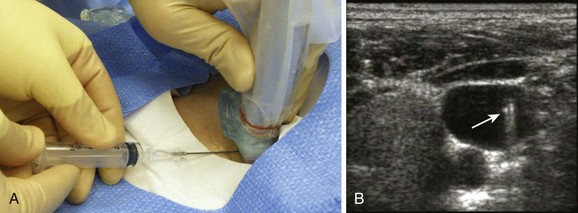
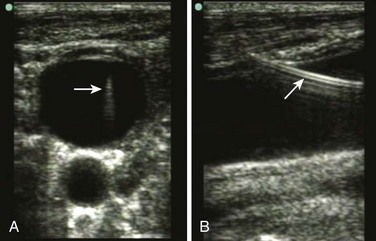
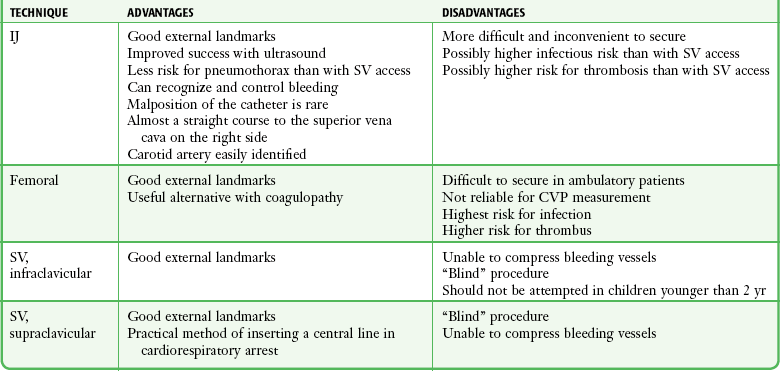
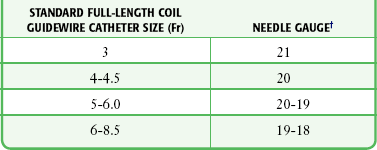
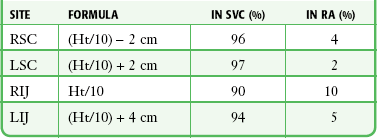
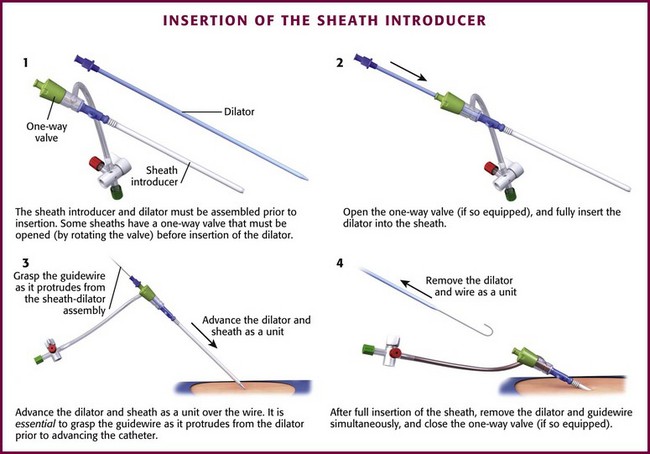
Chapter 22 Central venous access remains a cornerstone of resuscitation and critical care in both the emergency department (ED) and intensive care unit. Advanced hemodynamic monitoring, rapid infusion of fluid, placement of transvenous pacemakers, and administration of selected medications all require reliable central venous access. Central venous catheterization has also gained acceptance in the resuscitation and treatment of critically ill children (see Chapter 19). Traditionally, the subclavian vein (SV), internal jugular (IJ) vein, and femoral vein have provided reliable and easily obtainable vascular access through the use of identifiable anatomic landmarks. Over the past decade, the increased availability of, training in, and provider competence in bedside ultrasonography have had a significant impact on the standard approach to both peripheral and central venous catheterization. Ultrasound-guided central venous catheterization has improved success rates, reduced complication rates, decreased the time required to perform the procedure, and resulted in overall cost savings. In 1667, the first known central venous catheter (CVC) was placed into a human IJ vein by Lower for a blood transfusion into the carotid artery of a sheep.1 Modern central venous catheterization heralds back to at least 1928 when Werner Forssmann, a 25-year-old German surgeon, performed a venous cutdown on his own left antecubital vein, inserted a ureteral catheter to a distance of 65 cm, and then climbed several flights of stairs to the radiology suite to confirm that it terminated in the right atrium. Although the hospital fired Dr. Forssmann for not obtaining permission, he went on to win the 1956 Nobel Prize for his pioneering efforts.1,2 Duffy reported a large series of femoral, jugular, and antecubital vein catheterizations in 1949.3 Aubaniac developed subclavian venipuncture while working on French Army casualties between 1942 and 1952.4 His infraclavicular SV approach was refined by Keeri-Szanto in 1956, and the supraclavicular approach to the vein was first described by Yoffa in 1965.5,6 Aside from Duffy’s earlier work, Hermosura (1966) and English (1969) are generally credited with scientific development of the percutaneous IJ approach.7 The most important advancement in modern CVC came in 1953 when the Swedish radiologist Sven Seldinger had the idea of advancing large catheters over a flexible wire that was inserted through a percutaneous needle.8,9 The role of central venous pressure (CVP) monitoring in the maintenance of optimal blood volume helped popularize central catheterization in the United States.10 This was accelerated by the advent of the pulmonary artery catheter, which was developed by Jeremy Swan and William Ganz in 1968.11 Swan, who was inspired by his observations of a sailing boat during a picnic with his children, developed a flow-directed balloon that allowed measurement of pulmonary artery pressure.12 The SV begins as a continuation of the axillary vein at the outer edge of the first rib. It joins the IJ vein to become the innominate (sometimes referred to as the brachiocephalic) vein 3 to 4 cm proximally. The SV has a diameter of 10 to 20 mm, is approximately 3 to 4 cm long, and is valveless. After crossing over the first rib, the vein lies posterior to the medial third of the clavicle. It is only in this area that there is an intimate association between the clavicle and the SV. The costoclavicular ligament lies anterior and inferior to the SV, and the fascia contiguous to this ligament invests the vessel. Posterior to the vein and separating it from the subclavian artery is the anterior scalene muscle, which has a thickness of 10 to 15 mm. The phrenic nerve passes over the anterior surface of the scalene muscle laterally and runs immediately behind the junction of the SV and the IJ vein. The larger thoracic duct (on the left) and the smaller lymphatic duct (on the right) pass over the anterior scalene muscle and enter the SV near its junction with the IJ vein. Superior and posterior to the subclavian artery lies the brachial plexus. The dome of the left lung may extend above the first rib, but the right lung rarely extends this high (Fig. 22-1). The IJ vein begins just medial to the mastoid process in the jugular foramen at the base of the skull and is formed by the inferior petrosal sinus and the sigmoid sinus. It runs inferiorly and passes under the sternal end of the clavicle to join the SV and form the innominate or brachiocephalic vein. At the level of the thyroid cartilage, the IJ vein, the internal carotid artery, and the vagus nerve course together in the carotid sheath just deep to the sternocleidomastoid (SCM) muscle. Within the carotid sheath, the IJ vein typically occupies the anterior lateral position and the carotid artery lies medial and slightly posterior to the vein. This relationship is relatively constant, but studies have found that the carotid artery may overlap the IJ. Note that normally the IJ vein migrates medially as it nears the clavicle, where it may lie directly over the carotid artery. When using the most common (central) approach, the IJ tends to be more lateral than expected.13,14 Furthermore, in 5.5% of those studied, the IJ vein may even be medial to the carotid artery.14–17 The relationship between the IJ vein and the carotid artery also depends on head position. Excessive head rotation can cause the carotid artery to rotate over the IJ vein.18,19 Generally, the right IJ is bigger than the left IJ because of its connection to the SV and the right atrium. The IJ vein can be pulsatile, but in contrast to the aorta, these pulsations are not palpable. When visualized, however, the presence of venous pulsations can give an indication of patency of the IJ vein to the right atrium. The IJ vein also changes size with respiration. Because of the negative intrathoracic pressure at end-inspiration, blood in the IJ vein is actually drawn into the right atrium and the diameter of the IJ vein shrinks. In contrast, at end-expiration the increased intrathoracic pressure will limit return of blood to the right atrium and the diameter of the IJ vein will increase. Another unique characteristic of the IJ vein is its distensibility. The IJ vein will enlarge when pressure in the vein is increased, such as when flow of blood back to the right atrium is obstructed, as with thrombosis. This distensibility can be advantageous for the placement of central venous access. Use of a head-down (Trendelenburg) position or a Valsalva maneuver will increase the diameter of the IJ vein and thereby increase the likelihood of successful puncture (Fig. 22-2). The femoral anatomy is less complex than that of the neck and shoulder and contains fewer vital structures. The femoral vein is most easily cannulated percutaneously in patients with a palpable femoral pulse. The femoral vein begins at the adductor canal (also known as Hunter’s canal) and ends at the inferior margin of the inguinal ligament, where it becomes the external iliac vein. It is contained within the femoral triangle (inguinal ligament, medial border of the adductor longus, and lateral border of the sartorius muscle). Medially, the femoral vein abuts a robust system of lymphatics. Laterally, the vein is intimately associated with the femoral artery. The femoral nerve courses down into the leg just lateral to the femoral artery. These relationships from lateral to medial can be remembered with the mnemonic NAVEL (nerve, artery, vein, empty space, lymphatics). Note that as the femoral artery and vein course down the leg within the femoral sheath, their side-by-side relationship frequently rotates such that the femoral artery may lie on top of the vein. Therefore, to avoid arterial puncture, keep cannulation attempts just under the inguinal ligament. When cannulating this vessel distal to the inguinal ligament, ultrasound guidance can be helpful to avoid arterial puncture (Fig. 22-3). Central venous access has several clinical indications (see Review Box 22-1). If necessary, any central venous approach could be used for each of these situations. However, certain approaches offer advantages over others in specific clinical settings. The clinical indications are discussed in detail in the following sections.20–22 For a period, pulmonary artery catheterization somewhat supplanted CVP monitoring; however, there is little evidence that this practice has any benefit with regard to patient mortality or quality of life. In the specific setting of resuscitation of patients in septic shock, CVP monitoring has reemerged as an important component of “early goal-directed therapy.”23,24 Continuous or episodic measurements of central venous O2 saturation play a prominent role in current protocols for the aggressive treatment of septic shock.23,24 Central venous catheterization is widely used as a vehicle for rapid volume resuscitation. Notwithstanding, short large-caliber peripheral catheters can be as effective as central access because of the properties of Poiseuille’s law, which states that the rate of flow is proportional to the radius of the catheter and inversely proportional to its length.3 To illustrate, the gravity flow rate of saline through a peripheral 5-cm, 14-gauge catheter is roughly twice that through a 20-cm, 16-gauge CVC. Consequently, placement of large-bore peripheral catheters is generally the fastest method of volume loading. The advent of thermoregulating high-volume rapid infusers affords the advantage of using central venous catheterization in the setting of severe hemorrhagic shock or hypothermia. The available systems can infuse blood warmed to 37°C through an 8.5-Fr introducer sheath 25% more rapidly than through a 14-gauge peripheral intravenous (IV) line and up to 50% faster than through an 18-gauge peripheral IV line.25 The Level 1 Rapid Infuser and the Belmont FMS 2000 are examples of modern systems with infusion rates as high as 1500 mL/min.25 Massive air embolism was a concern with early rapid infusers, but safety precautions have now been engineered to prevent this. Still, if the catheter is misplaced, fluid or blood can be rapidly infused into the thorax, mediastinum, or peritoneum with serious consequences. The predictable anatomic locations of the subclavian and femoral veins and the speed with which they can be cannulated have prompted their use in cardiac arrest and other emergency situations. The need for a central line during cardiopulmonary resuscitation (CPR) is controversial.26–28 When achieved easily, central venous cannulation, especially via the IJ or SV route, is preferred over peripheral venous access because it provides a rapid and reliable route for the administration of drugs to the central circulation of patients in cardiac arrest. With resuscitation for aortic catastrophes or thoracoabdominal trauma, two CVCs, “one above and one below” the diaphragm, are often used. Patients with a history of IV drug use, major burns, chronic disease, dehydration, or morbid obesity and those who require long-term access may have inadequate peripheral IV sites. Central venous cannulation may be indicated as a means of venous access in these patients even under nonemergency conditions.29 More recently with the use of ultrasound, deep brachial, axillary, and basilic vein cannulation may be attempted before central venous catheterization. This approach avoids the complications that can be associated with central venous access. Additionally, serial lactate levels may help guide early goal-directed resuscitation. With an imbalance in oxygen supply (Do2) and consumption (Vo2), tissue hypoperfusion and hypoxia lead to anaerobic metabolism. The final product of this process is lactate. Arterial lactate levels would best represent overall perfusion since such samples contain blood coming from the pulmonary veins, superior vena cava (SVC), and inferior vena cava (IVC). Peripheral lactate preferentially reflects perfusion and metabolism in the compartment from which the blood was drawn, but not overall perfusion. Arterial and central venous lactate correlate closely more than 96% of the time, whereas peripheral venous lactate and arterial lactate correlate only 87% of the time.30 Central catheters, though safer than peripheral IV lines, are not immune to extravasation; indeed, fatal cases have been reported if the catheter becomes wedged up against the vessel wall, valves, or endocardium.31 Strategies to avoid this complication include delivering vesicant drugs only through the distal ports or reconfirming that the proximal port is safely in the vein by aspirating blood through it.31 Other indications for central venous access include insertion of a pulmonary artery catheter or transvenous pacemaker, cardiac catheterization, pulmonary angiography, and hemodialysis. A pulmonary artery catheter can be valuable for determining fluid and hemodynamic status in the critically ill. Its widespread use in the 1980s and 1990s drew heavy criticism because data showing a benefit in patient-oriented outcomes were lacking. Pulmonary artery catheters have subsequently lost popularity and should be used only when the diagnostic benefits outweigh the potential risks.32,33 Catheters such as the Uldall and Quinton devices can be inserted within minutes, thereby permitting emergency or short-term hemodialysis. However, these catheters are very large and relatively stiff and have been known to perforate the vena cava or atrial walls, with fatal outcomes.34,35 Extra caution should be applied during their insertion, possibly under ultrasound or fluoroscopic guidance. General contraindications to the various techniques of central venous access are presented in Review Box 22-1. Table 22-1 lists the general advantages and disadvantages with each approach. Most contraindications listed are relative and should be viewed in the context of the patient’s overall condition, urgency of need, and availability of alternative options for vascular access. Perhaps the only true absolute contraindication is insertion of catheters impregnated with antibiotics (most commonly tetracycline, rifampin, or chlorhexidine) if the patient has a serious allergy to the drug.36,37 Local cellulitis and distorted local anatomy or landmarks are relative contraindications to any access route. Each technique is contraindicated in patients with distorted local anatomy or landmarks preventing safe insertion. Insertion of catheters through freshly burned regions, though somewhat challenging, is not associated with a higher incidence of infection until approximately 3 days after the burn, when bacterial colonization accelerates.38,39 One of the more commonly encountered impediments to CVC placement is morbid obesity.40 Surface landmarks in the neck are often obscured, and an abdominal pannus can block the femoral access site and consequently require deeper insertions and steeper angles. An ultrasound-guided IJ approach is safer under these circumstances.40 Insertion of another catheter on the same side as a preexisting one risks the complication of entrapment.41 Combativeness is an important factor in the decision to place a CVC because the risk for mechanical complications greatly increases in uncooperative patients. Sometimes it is best to sedate and intubate critically ill patients before attempting central venous catheterization. Other relative contraindications include conditions predisposing to sclerosis or thrombosis of the central veins, such as vasculitis, previous long-term cannulation, or illicit IV drug use via any of the deep venous systems. TABLE 22-1 Advantages and Disadvantages of Central Venous Access Techniques CVP, central venous pressure; IJ, internal jugular; SV, subclavian vein. Coagulopathy is a frequent concern surrounding insertion of a CVC, with the overall risk for clinically significant hemorrhage in these patients approximating 2%.42 A transfusion of fresh frozen plasma is commonly used to correct any existing coagulopathy. However, a recent review concluded that if good technique is used, correction of coagulopathy is not generally required before or during the procedure.43 Mumtaz and coworkers found that even in thrombocytopenic patients (platelet count <50 × 109/L), bleeding complications occurred about 3% of the time and were limited to bleeding at the insertion site44; these complications were managed with additional sutures. Although the occasional patient may require a blood transfusion or replacement of clotting factors if a hemorrhagic complication arises, prophylactic correction of an abnormal international normalized ratio or platelet count before the procedure is not routinely necessary.43–45 Risk can be further reduced in coagulopathic patients with the use of ultrasound-guided placement techniques.14,46–49 SV access is contraindicated in patients who have previously undergone surgery or sustained trauma involving the clavicle, the first rib, or the subclavian vessels; those with previous radiation therapy involving the clavicular area; those with significant chest wall deformities; and those with marked cachexia or obesity. Patients with unilateral deformities not associated with pneumothorax (e.g., fractured clavicle) should be catheterized on the opposite side. Subclavian venipuncture is not contraindicated in patients with penetrating thoracic wounds unless the injuries are known or suspected to involve the subclavian vessels or SVC. Generally, cannulate the vein on the same side as the chest wound to avoid the possibility of bilateral pneumothoraces. When (preexisting) SV injury is suspected, cannulate on the opposite side. Exercise greater caution when placing a CVC in the SV in coagulopathic patients because this vessel is not compressible. Formerly, subclavian venipuncture was not recommended for use in small children, but in experienced hands it has been demonstrated to be safe.50–52 Cervical trauma with swelling or anatomic distortion at the intended site of IJ venipuncture is the most important contraindication to the IJ approach. Likewise, the presence of a cervical collar is problematic. Although bleeding disorders are relative contraindications to central venous cannulation, the ultrasound-guided IJ approach is preferred over the SV route because the IJ site is compressible. However, prolonged compression of the artery to control bleeding could impair the cerebral circulation if collateral blood flow is compromised. In a study by Oguzkurt and colleagues, only minor bleeding complications occurred in less than 2% of patients after ultrasound-guided IJ catheterization.47 In the setting of severe bleeding diatheses, the ultrasound-guided femoral approach is an acceptable alternative. Ultrasound-guided IJ placement is preferred in patients with abnormal anatomy from previous IJ trauma, small IJ vessels, and morbid obesity. Historically, carotid artery disease (obstruction or atherosclerotic plaque) is a relative contraindication to IJ cannulation because inadvertent puncture or manipulation of the artery could dislodge a plaque. If a preceding SV catheterization has been unsuccessful, the ipsilateral IJ route is generally preferred for a subsequent attempt. In this manner, bilateral iatrogenic complications can be avoided. Contraindications to femoral cannulation include known or suspected intraabdominal hemorrhage or injury to the pelvis, groin, iliac vessels, or IVC. Additionally, avoid the femoral approach when known or suspected deep venous thrombosis is present. Palpation for femoral pulsations during CPR is difficult, and the pulsations are often venous rather than arterial.28,53 Ultrasound-guided catheterization of the femoral vein during CPR is more successful and less likely than the standard landmark-oriented approach to incur inadvertent arterial puncture.28 The most commonly used method for central venous cannulation is the Seldinger (guidewire) technique, in which a thin-walled needle is used to introduce a guidewire into the vessel lumen. Seldinger originally described this technique in 1953 as a method of placing a catheter for percutaneous arteriography.17 The Seldinger technique is illustrated in Figure 22-9. To obtain vascular access, insert a small needle into the intended vessel. Once the introducer needle is positioned within the lumen of the vessel, thread a wire through the needle and then remove the needle. The wire, now within the vessel, serves as a guide over which the catheter is inserted. Although the Seldinger technique involves several steps, it can be performed quickly once mastered. More importantly, this technique broadens the application of central venous cannulation by permitting the insertion of standard infusion catheters, multilumen catheters, large-bore rapid infusion systems, introducer devices, hemodialysis devices, and even peripheral cardiopulmonary bypass cannulas. Given this flexibility, the use of Seldinger-type systems is advantageous despite their greater cost. Ultrasound guidance has revolutionized the cannulation of central veins. As with all anatomic structures in the human body, veins are highly variable in their location. Not surprisingly, research has demonstrated that the ability to see the internal structure’s location and proximity to other structures greatly increases the safety and success rate while decreasing the time required to perform the procedure.46–49,54–56 These advantages have been recognized by national organizations. In a report from the Agency for Healthcare Research and Quality (AHRQ), use of ultrasound guidance was listed as one of the top 10 ways to reduce morbidity and mortality.57 Many hospitals now require the use of ultrasound guidance for the placement of all CVCs. The basic materials required for central venous cannulation are shown in Review Box 22-1 and are discussed in further detail below. The catheter may be a component in a guidewire system or may be of the over-the-needle variety (the other widely used method for catheter placement). Several types of CVC Seldinger-type prepackaged kits are commercially available, and the variations in each kit are discussed in the next section. Preparation and organization of equipment ahead of time are imperative for a successful procedure. Most catheters now come from the manufacturer in convenient sterile kits. We strongly recommend stocking all additional equipment such as sterile gowns, gloves, and drapes in a dedicated “central line cart.” This is a fundamental part of the “bundling” practice that has been shown to reduce the search for supplies, improve compliance with full-barrier technique, and subsequently decrease catheter-related infections.58–63 Sterile barrier precautions with cap, face mask, sterile gown, and gloves should be used at all times during insertion of CVCs.61,64,65 Historically, many clinicians preferred to first locate the position of a central vein with a small exploratory or “finder” needle rather than directly cannulating the vein with a larger needle to accommodate a guidewire or catheter. This practice is less practical for the SV approach and has largely been replaced with the use of bedside ultrasound. Ultrasound-guided CVC placement allows the provider to survey the anatomy before the procedure, guide insertion of the needle into the correct vessel, and confirm placement of the catheter in the vessel.14,47–49 See the Ultrasound Box. Virtually any needle or catheter can be used to introduce a guidewire into a vessel, but there are advantages to using needles specifically designed for passage of a guidewire. These needles must be large enough to accommodate the desired wire yet be as small as possible to minimize bleeding complications. The introducer needles provided with CVCs or introducer devices are usually thin walled to maximize lumen size relative to the overall needle diameter. If a needle that is not thin walled is used, choose a size that is 1 gauge smaller (larger bore) than that listed in Table 22-2. If unsure, simply test the equipment first to ensure compatibility. TABLE 22-2 Needle Sizes for Venous and Arterial Catheters* *Any size of catheter from 3.0 to 8.5 Fr may be introduced with a 22-gauge needle if a solid wire (e.g., Cor-Flex, Cook Critical Care) is used. †All needle gauges are for thin-walled needles only, the type supplied in central line kits. Standard needles may have a uniformly straight-bore lumen throughout their length. A wire passing into a straight needle may encounter an obstacle at the proximal end. The proximal end of a Seldinger needle incorporates a funnel-shaped taper that guides the wire directly into the needle (Fig. 22-4). It is advisable to use a non–Luer-Lok or slip-tip type of syringe because the added twisting that is required to remove a Luer-Lok syringe from the introducer needle may dislodge a tenuously placed needle. Safety syringe systems exist that permit passage of the wire without removal of the aspirating syringe by using a central tunnel in the barrel. This device incorporates a hollow syringe through which the guidewire can pass directly into the introducing needle without detachment. It also reduces the risk for air embolism, which can occur when the needle is open to air. It is not uncommon for the wire to become snagged at the junction of the safety syringe and the needle hub. In this case, simply remove the syringe and insert the wire directly. Two basic types of guidewires are used: straight and J shaped. Straight wires are for use in vessels with a linear configuration, whereas J-wires are for use in tortuous vessels. Both wires have essentially the same internal design (Fig. 22-5). The flexibility of the wire is the result of a stainless steel coil or helix that forms the bulk of the guidewire. Within the central lumen of the helix is a straight central core wire, called a mandrel, that adds rigidity to the steel coil. The mandrel is usually fixed at one end of the helix and terminates 0.5 and 3.0 cm from the other end to create a flexible or floppy tip. Wires are also available with two flexible ends, one straight and the other J shaped. The flexible end of the guidewire allows the wire to flex on contact with the wall of a vessel. If the contact is tangential, as with an infraclavicular approach to the SV, a straight wire is generally preferred. If the angle is more acute, as with an external jugular approach to the SV, or if the vessel is particularly tortuous or valves must be traversed, a J-shaped wire may be used. The more rounded leading edge of the J-wire provides a broader surface to manipulate within the vessel and decreases the risk for perforation. This is especially advantageous when attempting to thread a wire through a vessel with valves. Many guidewires also contain a straight safety wire that runs parallel to the mandrel to keep the wire from kinking or shearing. It is important to emphasize that guidewires are delicate and may bend, kink, or unwind. A force of 4 to 6 lb may cause a wire to rupture. Wires should thread easily and smoothly and never be forced; the worst complications of CVC placement are associated with the application of excessive force across parts of the apparatus that are not threading smoothly.66 If a wire is not passing easily, withdraw the wire and the introducer needle as a single unit. Embolization of portions of the guidewire is possible, and sharp defects in the wire may perforate vessel walls (Fig. 22-6). If one encounters a good flash of blood but cannot readily manipulate the wire, this may indicate that the outer wire coils are entrapped against the proximal sharp edge of the needle bevel. The J can be straightened remotely by applying gentle force on the wire in each direction, which may allow retrieval of the wire.55 Wires should be inspected for small defects such as kinks, sharp ends, or spurs before use and especially after a failed attempt. Wires may be threaded into the introducer needle hub more easily by using the plastic sleeve attached to the wire as shown in Figure 22-5C. A number of different catheter and introducer devices have been developed, and the method of passage into the vessel varies accordingly. The functions of catheters have become more sophisticated as well, most notably for continuous monitoring of central venous oxygen saturation and cardiac output. Generally, one can place single-, double-, and triple-lumen catheters by sliding the catheter directly over a guidewire into the intended vessel (Fig. 22-7A). Catheter insertion lengths are listed in Table 22-3. Larger catheters or devices without lumens can be introduced with a sheath-introducer system. Over-the-needle catheters can be introduced once intravascular placement is attained. TABLE 22-3 Formulas for Catheter Insertion Length Based on Patient Height and Approach From Czepizak C, O’Callaghan JM, Venus B. Evaluation of formulas for optimal positioning of central venous catheters. Chest. 1995;107:1662. Reproduced by permission. The Desilets-Hoffman–type sheath introducer became available in 1965 to aid in arteriography procedures that require many catheter changes. This device is commonly but incorrectly termed a “Cordis,” which is a proprietary trade name. The sheath-introducer unit includes two parts, an inner dilator and an outer sheath as shown in Figure 22-7B. The dilator is rigid with a narrow lumen to accommodate the guidewire. It is longer and thinner than its sheath and has a tapered end that dilates the subcutaneous tissue and vessel defect created by the needle. The sheath (or introducer catheter when used as a cannula for inserting Swan-Ganz catheters, transvenous pacemakers, or other devices) has a blunt end and is simply a large-diameter catheter. Special catheters have been developed to prevent bacterial contamination and line sepsis.37,67,68 These catheters are impregnated with either antiseptics (silver sulfadiazine and chlorhexidine) or antibiotics (minocycline, rifampin, or cefazolin) to reduce bacterial colonization and microbial growth. Also, heparin-coated catheters are available that prevent fibronectin binding, thereby inhibiting the formation of bacterial biofilm on the catheter’s surface. These catheters can decrease catheter-associated infection (CAI) significantly and are cost-effective when the prevalence of CAI is greater than 2%.42 They should be avoided in patients with a history of heparin-induced thrombocytopenia.69 Minocycline- and rifampin-impregnated catheters are currently considered to be the most effective.37,67 Other interventions that decrease central line infections include the use of full sterile barrier precautions,61,65 skin preparation with chlorhexidine solution,61–63,70 and placement by experienced physicians.65,71–73 Many different catheters are currently manufactured. Although this leads to great flexibility in choice and cost, it often results in confusion when a clinician is handed an unfamiliar catheter during an emergency. It is best to use one brand routinely and to ensure that all medical personnel are thoroughly familiar with its use.74 When possible, discuss the procedure with the patient and obtain written informed consent. Place the patient and yourself in an appropriate position for the specific vessel being accessed. If available, perform an ultrasound survey to identify the patient’s anatomy, ensure vessel patency, and confirm the puncture site (Fig. 22-8). Ultrasound-guided CVC placement has been shown to decrease procedure times, as well as complication rates.46–49 Additionally, compliance with a central line bundling policy has been shown to significantly decrease central line–associated bloodstream infections.60–63 Prepare and drape the puncture site while maintaining sterile technique, and observe universal precautions throughout the procedure (Fig. 22-9, steps 1 and 2). A gown, surgical cap, mask, eye protection, and sterile gloves should be worn throughout the procedure when possible. When performing ultrasound-guided placement of a CVC, ensure that a sterile transducer sheath and sterile transducer gel are used during the procedure (see Fig. 22-9, step 3). Using an assistant will prove valuable in patient preparation, maintenance of sterility, and handling of the equipment. When performing ultrasound-guided placement of a CVC, begin with an ultrasound survey of the target vein, surrounding structures, and venipuncture location, as shown in Figure 22-8. Veins can easily be distinguished from the nearby artery by applying external pressure with the transducer. Veins collapse completely with pressure, whereas arteries may deform but do not usually collapse. Occasionally, the vein does not collapse with pressure. If this occurs, a thrombus may be present in the vein or the structure has been misidentified. If a suspected vein does not collapse with pressure, it is not an appropriate vessel for cannulation. If available, Doppler functions may also be helpful in the differentiation of veins and arteries. Select a venipuncture location where branching of the vein will allow the shortest path of the needle, will not obstruct passage of the catheter, and will not allow inadvertent puncture of other vital anatomic structures. (See Chapter 66 for additional information and descriptions of the ultrasound technique.) Prepare the catheter for insertion by flushing each lumen with sterile normal saline. Anesthetize the insertion site with lidocaine or bupivacaine (see Fig. 22-9, step 5). Attach a small syringe to an introducing needle that is large enough to accommodate the guidewire. Insert the needle and syringe together. Slowly advance the needle into the vein and apply steady negative pressure on the syringe (see Fig. 22-9, step 6). When performing ultrasound-guided CVC placement, follow the needle trajectory in the soft tissue and observe penetration of the vessel. If the tip of the needle is not visualized at all times with ultrasound, the needle may be passed into structures other than the vein. The key concept in using ultrasound guidance for venous access is to visualize the tip of the needle at all times during cannulation (Fig. 22-10). Once the tip of the needle enters the vessel lumen, blood will be aspirated freely. Stabilize the needle hub to prevent movement of the needle and displacement of the tip from the vessel, and remove the syringe. The need to disconnect the syringe can be eliminated by use of the Arrow Safety Syringe. After removing the syringe, cap the needle hub with your thumb before passing the guidewire to minimize the potential for air embolism. Introduce the flexible end of the guidewire into the hub of the needle (see Fig. 22-9, step 7). It may be easier to introduce the J-wire by advancing the plastic sleeve contained in the kit onto the floppy end of the wire to straighten the J shape. This straightened end is then introduced into the needle hub. The guidewire should thread smoothly through the needle into the vessel without resistance. Do not force the wire if resistance is encountered, but remove it from the needle and reattach the syringe to aspirate blood and reconfirm intravascular needle placement. It is important for the wire to slip easily from the needle during removal. If resistance to removal of the wire is felt, the wire and needle should be removed as a single unit to prevent shearing of the wire and resultant wire embolism. It has been recommended by some that no wire should ever be withdrawn through the introducing needle.75 Although there are no clinical data to support this recommendation and newer wires are stronger and more resistant to shearing, it represents the safest course of action. The recommendation to remove the needle and wire as a unit is sometimes disregarded because of reluctance to abandon a potentially successful venipuncture. The clinician performing the procedure must use both caution and good judgment to determine the best course of action but should not withdraw the guidewire against resistance. Manipulation of the wire within an introducer needle should be done only with standard coil guidewires. Solid wires (such as Cor-Flex Wire Guides from Cook Critical Care) have a small lip at the point at which the flexible coil is soldered to the wire. This lip can become caught on the edge of the tip of the needle and shear off the coil portion of the wire. Solid wires must thread freely on the first attempt or the entire wire and needle assembly must be removed. Keep backup wires on hand. If threading easily, advance the guidewire until at least one quarter of the wire is within the vessel. The further into the vessel the wire extends, the more stable its location when the catheter is introduced. However, advancing the guidewire too far may result in ventricular ectopy secondary to endocardial irritation, myocardial puncture leading to tamponade, or entanglement in a previously placed pacemaker, internal defibrillator, or IVC filter. In both the left and right IJ vein and infraclavicular SV approaches, fluoroscopic study during passage of the guidewire has determined the mean distance from skin to the SVC-atrial junction to be 18 cm.75 This distance has been recommended as the greatest depth of guidewire insertion for these approaches. It should be noted that 18 cm is not necessarily the appropriate final depth for the catheter being placed (see discussion below). Occasionally, a wire threads easily past the tip of the needle and then suddenly will not advance farther. If the introducer needle demonstrated free return of blood at the time of wire entry and the initial advancement of the wire met no resistance, the two options are to halt the procedure or seek confirmation of wire position. The guidewire within the lumen of the vessel can be visualized and confirmed via cross-sectional and longitudinal views on ultrasound. Alternatively, the needle may be removed, the wire fixed in place with a sterile hemostat, and a radiograph taken to confirm the position of the wire.75,76 A freely advancing wire may suddenly stop once it is well within a vessel if the vessel makes an unsuspected bend or is being compressed or deviated by another structure, such as a rib or muscle. This seems especially common with the infraclavicular approach to the SV and can sometimes be remedied by a more lateral approach. Once the wire is placed into the vessel, remove the needle in preparation for passage of the catheter (see Fig. 22-9, step 8). Proper positioning of the guidewire within the vessel lumen can be confirmed by cross-sectional and longitudinal ultrasound imaging (Fig. 22-11).76 This can be done at any point while inserting the wire to ensure that the correct vessel has been cannulated and that puncture of the posterior wall has not occurred. This technique can be quite useful when resistance is encountered while feeding the guidewire. A small skin incision is required at the site of the wire to widen the opening (see Fig. 22-9, step 9). Make the incision approximately the width of the catheter to be introduced and extend it completely through the dermis. When placing soft multiple-lumen catheters, the tissue must be dilated from the skin to the vessel before placement of the catheter. Thread the guidewire through the distal opening of the rigid dilator until it extends through the proximal end of the dilator (see Fig. 22-9, step 10). The wire must always be visibly protruding from the end of the dilator or catheter during insertion to avoid inadvertent advancement of the wire into the circulation and potential loss of the wire. While maintaining control of the guidewire proximally, thread the dilator over the wire into the skin with a twisting motion. Advance the rigid dilator only a few centimeters into the vessel, and then remove it. Once the dilator is removed, thread the soft catheter into position over the wire. Placement of multiple-lumen catheters requires identification of the distal lumen and its corresponding hub. Find the distal lumen at the very tip of the catheter. The corresponding hub is usually labeled “distal” by the manufacturer. If there is any confusion, inject a small amount of sterile saline through each hub until it is observed exiting the distal lumen. Once the distal hub is identified, remove its cover cap to allow passage of the guidewire. Place the catheter by threading the guidewire into the distal lumen and advancing it until it protrudes from the identified hub (see Fig. 22-9, step 11). It is imperative that the guidewire protrude from the catheter hub and that it be firmly grasped as the wire and catheter are advanced. If the wire does not protrude from the proximal end of the catheter, withdraw the wire at the skin entry point until it protrudes enough to be grasped. While maintaining control of the guidewire proximally, advance the catheter into the vessel to the desired catheter insertion length (see Fig. 22-9, step 12). Ultrasonography can be used to verify proper catheter placement. After insertion of the catheter the wire must be removed (see Fig. 22-9, step 13) and the catheter must be anchored to the skin with sutures. When removing the wire from a catheter it must slip out easily. If any resistance is met, remove both the wire and the catheter as a single unit and reattempt the procedure. A common cause of a “stuck wire” is a small piece of adipose tissue wedged between the wire and the lumen of the catheter. Avoid this problem by creating a deep enough skin nick and adequate dilation of the tract before inserting the catheter. When placing a single-lumen, Desilets-Hoffman sheath-introducer system, the dilator and larger single-lumen catheter are inserted simultaneously as a dilator-sheath unit. The dilator-sheath unit must first be assembled by inserting the dilator through the catheter’s diaphragm (Fig. 22-12, step 2). When assembled correctly, the dilator “snaps” into place within the lumen of the sheath and protrudes several centimeters from the distal end of the catheter. Figure 22-12 Insertion of the sheath introducer. Insertion of a sheath introducer varies slightly from that for a triple-lumen catheter—the dilator and the catheter are inserted simultaneously as depicted. The remainder of the steps are analogous to those in Figure 22-9. Once inserted, sheath introducers facilitate the placement of devices such as pulmonary artery catheters and transvenous pacemakers. After successful guidewire placement and after the skin incision is made, thread the dilator-sheath assembly over the wire (see Fig. 22-12, step 3). It is imperative that the guidewire protrude from the proximal end of the dilator-sheath assembly and that it be firmly grasped as the wire and unit is advanced. If the wire does not protrude from the proximal end of the assembly, withdraw the wire at the skin entry point until it protrudes enough to be grasped. While maintaining control of the guidewire proximally, advance the assembly through the skin with a twisting motion until it is within the vessel. Grasp the unit at the junction of the sheath and dilator. This prevents the thinner sheath from kinking or bending at the tip or from bunching up at the coupler end. Keep the assembly intact and advance it through the skin to the hub. Once the catheter is placed, remove the wire and dilator from the sheath simultaneously (see Fig. 22-12, step 4). When removing the wire and dilator, the dilator must “unsnap” from the sheath unit, and the wire must slip out easily. Once the single-lumen sheath-introducer catheter is placed correctly, it may be used to facilitate the placement of additional intraluminal devices such as a pulmonary artery catheter, transvenous cardiac pacemaker, or additional multiple-lumen catheter. At times, critically ill patients who require initial large-volume resuscitation will later require multiple medications and therapies that dictate the need for a multiple-lumen catheter. An alternative method of placing a multiple-lumen catheter is to thread the catheter through a standard Desilets-Hoffman sheath-introducer system. It is important to consider the depth of insertion of the catheter (see Table 22-3). The proper depth of catheter insertion is site specific (see below). After successful CVC placement, the catheter should be anchored to the skin with sutures (see Fig. 22-9, step 15). Each port should be immediately capped and flushed with a saline solution (see Fig. 22-9, step 14). The catheter insertion site should be dressed appropriately and all sharp implements disposed of in appropriate receptacles (see Fig. 22-9, step 16). Replacement of an existing catheter begins with selecting a guidewire longer than either of the devices to be exchanged. Use meticulous aseptic technique.70 Insert the guidewire into the existing CVC until a few centimeters of wire is protruding from the proximal end. With one hand holding the wire securely, remove the catheter and wire as a single unit until the tip of the catheter just clears the patient’s skin. Grasp the wire at the point where it exits the skin and only then release the wire at the other end. Then slide the catheter off the wire and insert the new device in the normal fashion. Exercise caution with this technique because catheter embolization can occur, especially if a catheter is cut to allow use of a shorter guidewire for the exchange. In patients without evidence of line sepsis, exchanging the guidewire does not increase the incidence of CAI if performed properly.70
Central Venous Catheterization and Central Venous Pressure Monitoring
Historical Perspective
Anatomy
IJ Vein
Femoral Vein
Indications
CVP Monitoring and Oximetry
Delivery of High-Flow Fluid Boluses and Blood Products
Emergency Venous Access and Inability to Achieve Peripheral Access
Routine Serial Blood Drawing
Infusion of Hyperalimentation and Other Concentrated Solutions
Other Indications
Contraindications
Subclavian Approach
IJ Approach
Femoral Approach
Procedure
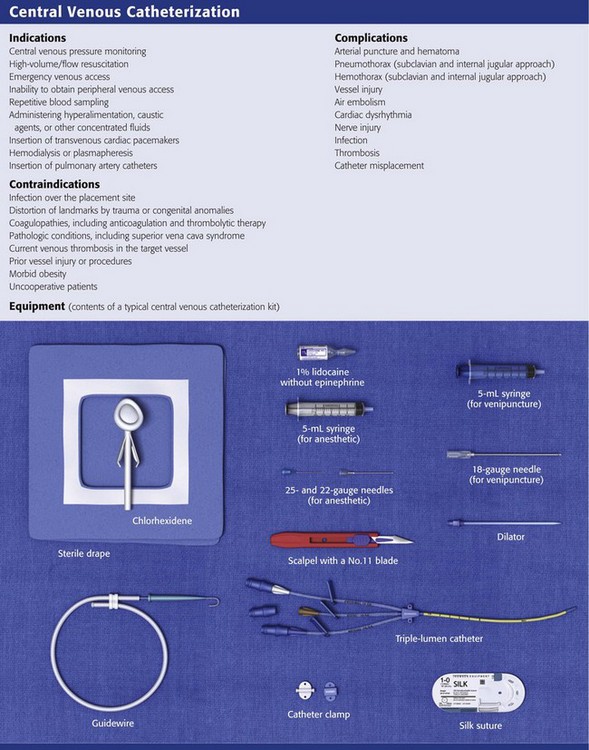
Equipment
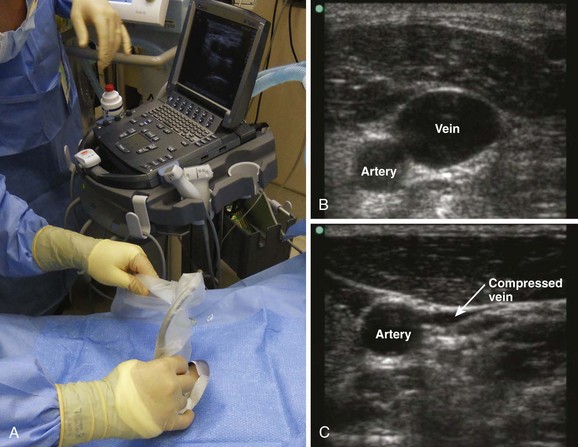
Ultrasound
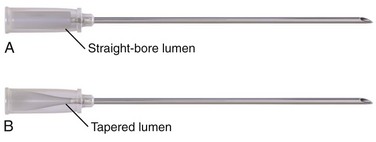
Needle
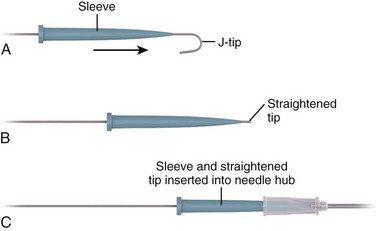
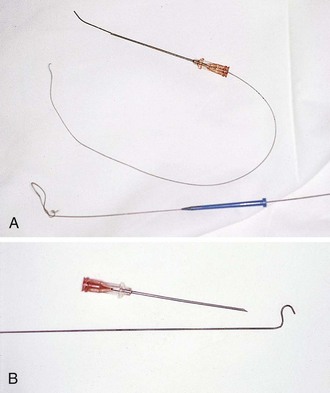
Guidewire
Catheters
Technique
Guidewire Placement with the Seldinger Technique
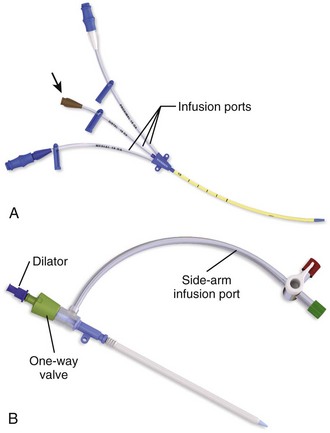
Sheath Unit and Catheter Placement
Replacement of Existing Catheters
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Veterian Key
Fastest Veterinary Medicine Insight Engine