Chapter 104Catastrophic Injuries
General principles for emergency first aid of severe distal limb injuries are as follows:
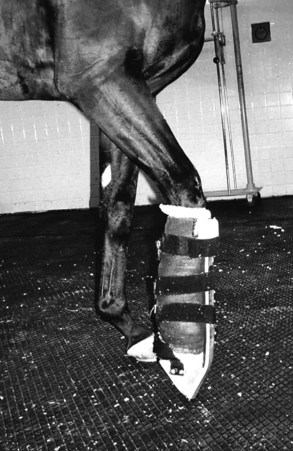
1 Immobilize with a dorsal splint that aligns the phalanges with the third metacarpal bone (McIII). This can be either with a prefabricated splint (e.g., Kimzey Leg Saver, Kimzey, Woodland, California, United States; Figure 104-1), or with a stave of split polyvinyl-chloride (PVC) pipe or something similar over a lightly padded bandage. The dorsal splint should extend from the proximal aspect of the McIII to the ground, covering the entire dorsal aspect of the hoof wall. The heel must be pulled upward toward the dorsal aspect of the splint to align the phalanges with the McIII. If a prefabricated splint is not available, a lightly padded bandage with a splint applied to the dorsal aspect of the metacarpal region, phalanges, and hoof serves the same purpose if the heel is kept elevated. This can be done by taping the heel and a heel wedge with nonelastic tape (e.g., duct tape) to the dorsally applied splint. Excessive padding should be avoided because it allows dorsal flexion within the bandage and shifting of the splint. A prefabricated splint is not ideal for all injuries because it may not provide medial-to-lateral stability, but it is usually adequate for first-aid stabilization. For injuries involving the upper limb a Robert Jones Bandage with splinting material incorporated within the bandage should be applied (see Chapter 86).
2 Tranquilize or sedate adequately to minimize further injury and allow examination. Xylazine or detomidine is usually adequate.
3 It is often difficult to know the exact nature of an injury without using diagnostic imagining, so do not make assumptions. If possible, immobilize the area of injury and transport the horse to a referral center for evaluation.
4 Do not hesitate to use parenteral antiinflammatory agents and analgesics. Many attending clinicians worry that antiinflammatory therapy may prompt an injured horse to use a limb, causing further damage; unless perineural analgesia is used, a horse with an injured limb will be unlikely to sustain further injury under the influence of parenteral medication.
5 If there is any skin damage, the horse should immediately be given broad-spectrum antimicrobial drugs intravenously.
6 Transport an injured horse in a tight stall, as tight as it can be, so that the horse can easily lean against side walls for support. Do not tie the head tightly. In general, horses with forelimb injuries should be transported facing backward, and those with hindlimb injuries facing forward.
The reader is referred to Chapter 86, and there are two excellent recent reviews that detail emergency stabilization of equine fractures.1,2
Types of Catastrophic Injuries
Traumatic Disruption of the Suspensory Apparatus
The hallmark clinical signs, fetlock drop and severe lameness, are seen in horses with complete disruption of any portion of the suspensory apparatus. The most common injury in both adult horses and foals is fracture of both proximal sesamoid bones (PSBs) (Figure 104-2
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


