Alison B. Clode
Cataract
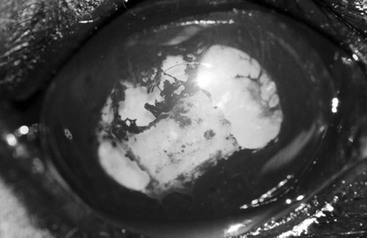
A cataract is an irreversible opacification of the crystalline lens caused by alterations in protein structure and binding associated with changes in lens metabolism. The clinical significance of a cataract depends on the underlying cause of the metabolic alterations, degree of obstruction of the visual axis, likelihood of progression, and presence or absence of additional ocular abnormalities. In consideration of each of these factors, a thorough classification of a cataract is necessary to determine the appropriate therapeutic options and prognosis for affected individuals. The criteria on which cataracts can be classified include etiology, age of the horse at onset, location within the lens, and extent of involvement of the lens (i.e., the maturity of the cataract). Cataracts can be primary or secondary. Primary cataracts are inherited in other species, but this has not been proven to occur in horses. More often, cataracts develop secondary to uveitis (most common), trauma, toxin exposure, or nutritional or metabolic alterations. Age of the horse at onset may be indicative of the underlying cause. Congenital cataracts, those diagnosed before 6 months of age, suggest an inherited cause or intrauterine exposure to toxins. Juvenile cataracts also may be inherited, whereas senile or geriatric cataracts may be a result of aging changes in the lens. If a distinct underlying cause for cataract development cannot be identified in an animal of breeding age, it is best to presume the cataract is inherited and to remove the horse from breeding programs. Classification of a cataract by location within the lens (anterior or posterior, axial [polar], paraxial, or peripheral; and capsular, cortical, or nuclear) and extent of involvement (incipient [<10%], immature [10% to 99%], mature [100%], or hypermature [resorption of lens and wrinkling of lens capsule]) determines the likely impact on vision as well as the potential progression of a cataract (Figures 142-1 and 142-2). In general, cataracts located within the lens nucleus are nonprogressive, whereas cortical cataracts are more likely to progress over a period of months to years. Cataracts located within the visual axis, even if relatively small, will have a disproportionately greater impact on vision, particularly when the pupil constricts in lighted conditions.

Clinical Signs and Diagnosis
Clinical signs observed by owners in association with cataracts include vision deficits involving one or both eyes, a change in ocular appearance, and signs of discomfort, such as squinting, tearing, and redness. Because these nonspecific clinical signs may be caused by a variety of disease processes, including corneal ulceration, uveitis, and glaucoma, diagnosis of cataracts necessitates a complete ophthalmic examination, ideally in a darkened area and with pharmacologic dilation (tropicamide 1%, 0.1 to 0.2 mL, administered topically, once to twice over 5 minutes). Initial assessment should include evaluation of the menace response, direct and consensual pupillary light reflexes, and dazzle reflexes. A horse with cataracts and a functioning retina should have positive reflexes, whereas the presence or absence of a menace response depends on the extent of the cataract. Illuminating the eye directly with a focal light source (direct illumination) reveals cataract as white opacification of the lens, whereas obtaining a tapetal reflection by shining the light into the eye from a few feet away (retroillumination; Figure 142-3) demonstrates cataract as areas in which the tapetal reflection is blocked. Application of fluorescein stain is indicated to thoroughly assess corneal health, which may be compromised in association with intraocular disease processes. Measurement of intraocular pressures (IOP) is also indicated because high IOP (>30 mm Hg) suggests glaucoma and lowered IOP (<10 mm Hg) suggests uveitis. Indirect or direct ophthalmoscopy should be performed; in an eye with an incipient or immature cataract, at least portions of the fundus should be visible, whereas the fundus will not be visible in an eye with a complete cataract.
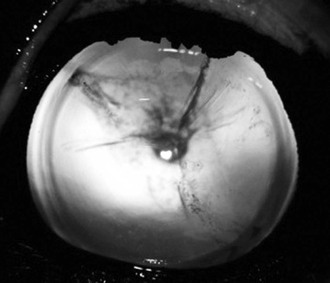
The diagnosis of cataract should prompt assessment for an underlying cause and concurrent ocular diseases. Obtaining a thorough history is imperative because the most common identifiable causes of cataracts in horses are uveitis and trauma. Any history of trauma, particularly penetrating ocular trauma, should be documented, regardless of when it occurred because trauma-induced cataracts may develop weeks to months after injury. Discerning whether cataracts are secondary to uveitis can be more difficult because cataracts may both result from and cause (lens-induced) uveitis. In general, chronic rather than acute uveitis is necessary to cause cataract formation, and cataracts in horses appear to result in less lens-induced uveitis than in other species. It is therefore more likely that uveitis precedes cataract development in most horses. Thorough inquiry into the nature of the ophthalmic disease, including specific signs, duration, previous treatments, and response to therapy, and evaluation for signs of systemic illness, as well as thorough ophthalmic examination, may assist in making this distinction. On ophthalmic examination, clinical signs specific for uveitis include ocular hypotony (IOP <10 mm Hg); miosis and resistance to pharmacologic mydriasis; aqueous flare, hyphema, or hypopyon, with or without keratic precipitates, which are accumulations of debris on the endothelium; and vitreal cellular debris. Although such signs indicate active uveitis, additional clinical signs suggestive of chronic uveitis include shrinking of the globe (phthisis bulbi), iridal hyperpigmentation, corpora nigra atrophy, cataract development (see Figure 142-2), lens subluxation or luxation, vitreal degeneration, and retinal degeneration or detachment. If signs suggestive of concurrent uveitis are not present and no history of trauma is known, it is most appropriate to presume cataracts are heritable.



