Chapter 5 Cardiovascular and Other Diseases
General Principles
History and Clinical Signs
Ferrets with cardiac disease show a variety of clinical signs similar to those observed in other species, including lethargy, exercise intolerance, weight loss, anorexia, ascites, coughing, and dyspnea.14,40,61 In addition, ferrets with cardiac disease may present with hind limb weakness. It is unclear why the hind limbs are preferentially affected compared with the front, but thromboembolic disease does not appear to be a cause. The diagnosis of cardiac disease may be an incidental finding in some ferrets; either these ferrets have compensated for mild cardiac disease or the owner has not noticed the often insidious signs.
Physical Examination
A thorough and systematic physical examination should be performed in ferrets with suspected cardiac disease. Examine the oral mucous membranes for color and refill time (less than 2 seconds is normal). Pale or cyanotic mucous membranes with a prolonged capillary refill time may be related to congestive heart failure (CHF) or reduced cardiac output. Jugular pulses may be visible in ferrets with right-sided CHF. Femoral pulses are palpated for quality, character, and the presence of any deficits. Pulses may be weak, irregular, or normal with cardiac disease. Bounding pulses are uncommon but could potentially be seen with a severe aortic insufficiency or a patent ductus arteriosus (PDA). Abdominal palpation of ferrets with heart disease may reveal ascites, hepatomegaly, and splenomegaly. Other findings on physical examination may include hypothermia, lethargy, generalized weakness, and dehydration.
Radiography
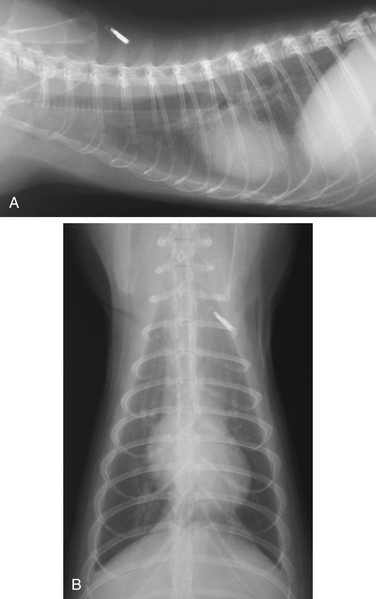
Standard two-view thoracic radiographs can yield important information for the diagnosis of cardiac disease and CHF. Because problems in the anterior mediastinum are common, the entire thorax should be included in the radiographs. Physical restraint is usually adequate to obtain radiographs, although a short dose of inhalant anesthesia or midazolam (0.3-0.5 mg/kg) may be used safely. The typical landmarks used for dogs and cats are inaccurate in ferrets because of the shape of the ferret’s thorax, which is elongated and flattened dorsoventrally.71 The normal ferret heart is more globoid in appearance than a dog or cat heart and is located approximately between the sixth and eighth intercostal spaces. The right ventricle is slightly in contact with the sternum (Fig. 5-1). If heart disease is present, the cardiac silhouette may appear enlarged, resulting in tracheal elevation, rounding of the cardiac silhouette, and increased sternal contact on the lateral view. On the ventrodorsal view, the heart may be elongated and widened, filling up a larger portion of the thorax.
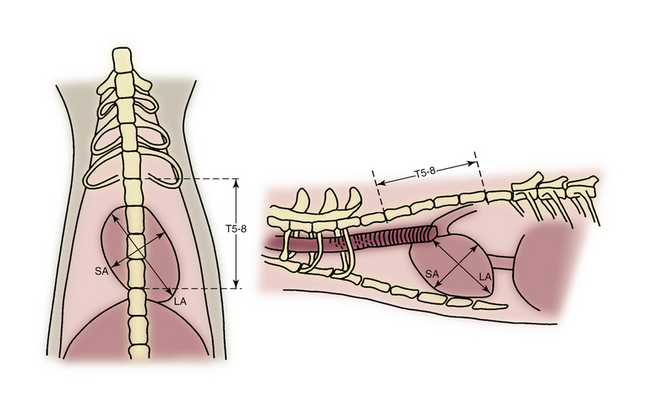
The size of the cardiac silhouette can be quantified by the use of a modified vertebral heart score (VHS).71 The technique involves measuring the length and width of the heart on the right lateral (RL) radiograph and expressing this measurement in units of vertebral length (Fig. 5-2). This method corrects for differences in size between ferrets. Because the presence of pericardial fat on the ventrodorsal (VD) view makes the edges of the cardiac silhouette more difficult to discern, the lateral view is more accurate. On the lateral view, the long axis of the heart is the length from the ventral border of the bifurcation of the trachea to the apex of the heart, and the short axis is the maximum length from the cranial to the caudal edges. On the ventrodorsal view, the long axis is the length of the heart along midline from the cranial border of the heart to the apex. The short axis is the maximum width of the heart measured perpendicular to the long axis. These measurements are compared with the length of the thoracic vertebrae (v), beginning with the cranial edge of the fifth thoracic vertebra (T5) to end of eighth thoracic vertebra (T8) and estimated to the nearest 0.25 vertebra. The heart length and width measurements in verterbral lengths from a single projection are then added to obtain a total score. The median VHS on the right lateral projection is 5.33 v, with a range of 5.23 to 5.47 v. The heart length plus width is 5.35 cm, with a range of 5.02 to 5.48 cm. The median VHS on the ventrodorsal view is 6.0 v, with a range of 5.73 to 6.15 v. Basically, the thoracic vertebrae in ferrets are 1 cm long between T5 and T8. Therefore you can measure length plus width, and the sum of these approximates the VHS.
Electrocardiography
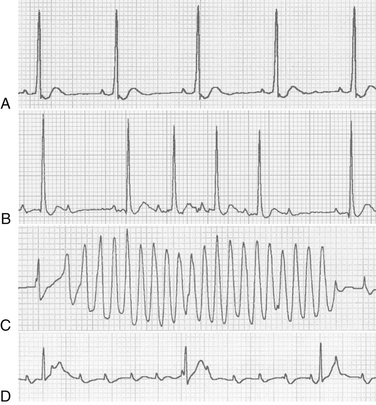
In ferrets, the electrocardiogram (ECG) is used primarily to determine the presence of abnormal rhythms and conduction disturbances. Reference values for ECGs in ferrets have been published and are summarized in Table 5-1.6,16,17,68 A variety of common arrhythmias have been seen in ferrets (Fig. 5-3). Sinus rhythm and sinus tachycardia are the most common rhythms seen on presentation with cardiac disease. Atrial and ventricular premature contractions may be recorded. Atrial fibrillation can occur in the presence of significant atrial enlargement. Sinus bradycardia can be associated with hypoglycemia, commonly seen in ferrets with insulinomas. Second-degree atrioventricular (AV) block can occur as a normal finding in healthy ferrets. High-grade second-degree AV block and complete (third-degree) AV block are rare. Complete AV block can be successfully treated by implanting an epicardial transdiaphragmatic pacemaker (Fig. 5-4). Other reported ECG changes include tall R waves, prolonged QRS complexes, and ST-segment depression.69
Table 5-1 Electrocardiographic Values for 52 Clinically Normal Ferretsa
| Parameter | Mean, or Mean ± SD (Range) (N = 25)6 | Value (N = 27)17 |
|---|---|---|
| Age (mo) | 10–20 | 5.2 |
| Male/female ratio | All male | 1.25 |
| Body weight (kg) | 1.4 ± 0.2 | Not available |
| Rhythm | ||
| Normal sinus | Not available | 67% |
| Sinus arrhythmia | Not available | 33% |
| Heart rate (beats/min) | 196 ± 26 (140–240) | 233 ± 22 |
| Mean electrical axis, frontal plane (degrees) | +86.1 ± 2.5 (79.6–90.0) | +77.2 ± 12.0 |
| Lead II measurements | ||
| P amplitude (mV) | Not available | 0.122 ± 0.007 |
| P duration (sec) | Not available | 0.024 ± 0.004 |
| PR interval (sec) | 0.056 ± 0.0086 (0.04–0.08) | 0.047 ± 0.003 |
| QRS duration (sec) | 0.044 ± 0.008 (0.035–0.06) | 0.043 ± 0.003 |
| R amplitude (mV) | 2.21 ± 0.42 (1.4–3.0) | 1.46 ± 0.84 |
| QT interval (sec) | 0.11 ± 0.02 (0.08–0.14) | 0.12 ± 0.04 |
a All ferrets were sedated with ketamine-xylazine.

The ECG is ideally done without sedation with the animal in right lateral recumbency (Fig. 5-5). The ECG clips can be flattened to produce a smooth surface that does not result in pinching. Because most ferrets object to the use of alcohol, ECG coupling gel (or ultrasound gel) is recommended. The ferret can be distracted by offering semisoft food such as a/d (Hill’s Pet Nutrition, Inc, Topeka, KS) or a nonsugary treat such as FerreTone (8 in 1, Islandia, NY) from a syringe while the ECG is being recorded.

Echocardiography
The echocardiogram remains the test of choice for diagnosing structural and functional cardiac abnormalities.46 In addition, the echocardiogram can be useful in identifying mediastinal masses and as an aid in detecting heartworm disease.65 It can often be obtained without the use of sedation. If sedation is required, either a short-acting injectable anesthetic or an inhalant anesthetic may be used. The echocardiogram is done with the animal in both right and left lateral recumbency. Imaging planes similar to those obtained in other species are recorded.77 Two-dimensional echocardiography provides an assessment of cardiac size and function. Standard M-mode measurements are obtained, including chamber dimensions, wall thickness, and indices of systolic function. Spectral Doppler imaging is used to quantitate the velocity of normal and abnormal blood flow. Color-flow Doppler echocardiography provides a visual inspection of blood flow direction and detection of turbulent flow, including valvular regurgitation. Echocardiographic reference values in the sedated ferret have been published and are summarized in Table 5-2.72 The echocardiogram is used in conjunction with good-quality thoracic radiographs to properly identify the severity of underlying cardiac disease and the presence of CHF.
Table 5-2 M-Mode and Doppler Echocardiographic Values for Normal Ferretsa
| Parameter | Value (Mean ± SD)72 |
|---|---|
| Interventricular septum end-diastole (IVSd) (cm) | 0.36 ± 0.07 |
| Interventricular septum end-systole (IVSs) (cm) | 0.48 ± 0.11 |
| Left ventricular free wall end-diastole (LVWd) (cm) | 0.42 ± 0.11 |
| Left ventricular free wall end-systole (LVWs) (cm) | 0.58 ± 0.99 |
| Left ventricular internal dimension end-diastole (LVIDd) (cm) | 0.88 ± 0.15 |
| Left ventricular internal dimension end-systole (LVIDs) (cm) | 0.59 ± 0.15 |
| Fractional shortening (%) | 33 ± 14 |
| Ejection fraction (%) | 69 ± 19 |
| Left atrial diameter (LA) (cm) | 0.71 ± 0.18 |
| Aortic diameter (AO) (cm) | 0.53 ± 0.10 |
| LA/AO (ratio) | 1.33 ± 0.27 |
| Pulmonary artery diameter (cm) | 0.48 ± 0.90 |
| Right ventricular free wall end-diastole (cm) | 0.12 ± 0.03 |
| Right ventricular internal dimension end-diastole (cm) | 0.38 ± 0.10 |
| Aorta maximum velocity (m/s) | 0.89 ± 0.20 |
| Pulmonary artery maximum velocity (m/s) | 1.10 ± 0.14 |
| Mitral valve E velocity (m/s) | 0.70 ± 0.10 |
| Mitral valve A velocity (m/s) | 0.52 ± 0.11 |
| Mitral valve velocity E/A ratio | 1.38 ± 0.32 |
a All ferrets were sedated with ketamine and midazolam (0.2 mg/kg).
Treatment
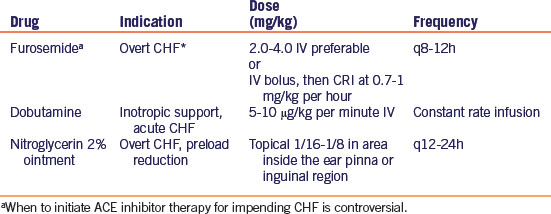
Basic therapeutic principles of CHF and cardiac disease are applied to ferrets. If a published ferret dose is not available, feline doses are often used as a starting point. Therapy for acute CHF (Table 5-3) focuses on improving oxygenation and reducing preload and afterload. Oxygen is provided by placing the animal in a closed cage or incubator with supplemental oxygen. Diuretics reduce preload by reducing blood volume.50 Furosemide is the most commonly used diuretic; it is most effective when given either intravenously or intramuscularly in the acute setting. Ferrets tolerate doses of 1 to 4 mg/kg every 8 to 12 hours. If respiratory rate does not decrease with pulse therapy with intravenous furosemide, consider treating with a constant rate infusion (CRI) of furosemide at a dose of 0.7 to 1 mg/kg per hour. Nitroglycerin 2% ointment is a venous dilator that can be applied to the skin in the axilla or inguinal area on a hairless body surface. Ferrets are sensitive to the hypotensive effects of nitroglycerin. Angiotensin-converting enzyme (ACE) inhibitors are given to reduce afterload by causing arterial vasodilation and to reduce preload by decreasing salt and water retention.37 The dose is usually started at 0.5 mg/kg PO given every 48 hours and then titrated up to every 24 hours if tolerated. In the first 24 to 48 hours of therapy, treatment with ACE inhibitors may result in hypotension or lethargy. The use of ACE inhibitors and concurrent diuretic therapy in ferrets with CHF can result in severe azotemia. Renal perfusion is reduced in CHF secondary to use of diuretics, decreased cardiac output, dehydration, and hypotension.28 If significant pleural effusion is present, resulting in an increased inspiratory effort, perform pleurocentesis and submit the fluid for fluid analysis and cytologic examination. In acute disease, monitor ferrets closely for respiratory rate and effort, mucous membrane color, heart rate and rhythm, body weight, and hydration as well as electrolyte, blood urea nitrogen (BUN), and creatinine values. Obtain serial radiographs to assess the response to therapy. Adjust medication dosages based on the listed monitoring parameters.
Table 5-3 Acute Dosages and Treatment Goals of Drugs Commonly Used to Treat Congestive Heart Failure in Ferrets
Chronic therapy typically includes furosemide, ACE inhibitors, digoxin, and a new positive inotrope, pimobendan (Vetmedin, Boehringer Ingelheim Vetmedica, St Joseph, MO) (Table 5-4). Furosemide is given orally at a dosage of 1 to 4 mg/kg q8-12h; ACE inhibitors are given at 0.5 mg/kg q24-48h as tolerated. Digoxin therapy is used as a positive inotrope and to depress AV nodal conduction with supraventricular arrhythmias.37 Digoxin elixir (0.05 mg/mL) is recommended because of the small doses required in ferrets. The recommended starting dosage is 0.01 mg/kg PO q12-24h.61 Calculated dosages for digoxin are based on lean body weight, usually 70% of body weight. Begin therapy once daily and then titrate up to twice daily depending on the clinical response and serum digoxin levels. Side effects of digoxin include inappetence, lethargy, vomiting, diarrhea, and arrhythmias.69 To date, no pharmacokinetic studies of digoxin in ferrets have been published. To measure digoxin levels, serum samples are taken approximately 6 to 8 hours after drug administration.69 Reference values for dogs and cats are extrapolated to interpret values in ferrets (0.8-2.0 ng/mL). Contraindications for the use of digoxin include significant azotemia, hypokalemia, bradyarrhythmias including AV block, and severe ventricular arrhythmias.37 In our clinic, digoxin is not used as the first-line positive inotrope because of the plethora of side effects and narrow therapeutic range. Pimobendan is used at a dosage of 0.625 to 1.25 mg/kg q12h. The positive inotropic effect is caused by the increased sensitivity of troponin C to calcium and also by inhibition of phosphodiesterase III. The latter mechanism results in vasodilation. In addition, this drug has neurohormonal effects, which include decreased levels of inflammatory cytokines (tumor necrosis factor [TNF] alpha, interleukin-1) and plasma epinephrine. Clinical studies in dogs reveal improved quality of life and survival with pimobendan therapy; whether or not this beneficial effect exists in ferrets is unknown. However, some experimental studies with pimobendan in ferrets have been performed.23,38,39,41
Table 5-4 Maintenance Dosages of Drugs Commonly Used to Treat Congestive Heart Failure (CHF) in Ferrets
Long-term management includes periodic monitoring for recurrence of CHF and changes in body weight, renal values, and heart rate and rhythm. If CHF recurs with standard therapy protocols, additional diuretics may be used, including thiazide diuretics or potassium-sparing diuretics such as spironolactone. Published feline dosages are used, and the dosage is titrated based on clinical response. Close monitoring of electrolytes after beginning more aggressive and mixed diuretic therapy is recommended. In ferrets with CHF receiving steroid therapy for lymphoma, spironolactone should be considered early in the disease process because of its effects on the aldosterone receptor in the distal renal tubule.50
The use of antiarrhythmic drugs is not well documented in ferrets. Atenolol titrated to effect can be given for many supraventricular and ventricular arrhythmias. Diltiazem can be used for many supraventricular arrhythmias to either reduce spontaneous occurrence or slow AV nodal conduction.36 Intravenous lidocaine can be used in ferrets with ventricular tachycardia; however, the dose should be reduced from that used in cats and then titrated to effect. With this class of antiarrhythmic drugs, close observation for the development of neurologic and gastrointestinal signs is essential.36
Dilated Cardiomyopathy
Dilated cardiomyopathy has been described in ferrets and has clinical characteristics similar to those observed in dogs and cats.14,20,40 The disease results in a dilated left ventricle, right ventricle, or both, with global systolic dysfunction. The cause of the disease in ferrets is not known; in one ferret, it was reported in association with a cryptococcal infection.20 Lethargy, dyspnea, anorexia, and weight loss are common complaints in the history. Physical examination findings can include hypothermia, heart murmur, tachycardia, pallor, weakness, or ascites. Pleural effusion is seen as an increased inspiratory effort with muffled heart sounds. Pulmonary edema is heard as moist rales and increased respiratory sounds. In many cases, both pulmonary edema and pleural effusion are present simultaneously, resulting in a combination of the clinical signs mentioned.
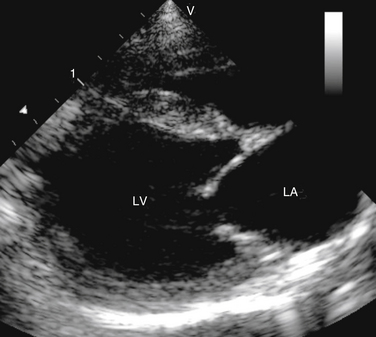
Echocardiography is used to make a definitive diagnosis of dilated cardiomyopathy. Typical echocardiographic changes are similar to those observed in other species.7,45,79 The left ventricle appears dilated, with increased end-systolic dimensions, and the left atrium is typically dilated (Fig. 5-6). Fractional shortening, a commonly used index of systolic function, is reduced. If the right side of the heart is involved, the right ventricle is dilated, right ventricular systolic motion is reduced, and the right atrium is enlarged. In advanced disease, mitral and tricuspid regurgitation secondary to dilation of the valve annulus is seen. Left ventricular outflow tract velocities can be normal or reduced.
A variety of ECG abnormalities may be present, including ventricular premature contractions, atrial premature contractions, atrial tachycardia, ventricular tachycardia, and atrial fibrillation.45,79
Therapy for acute clinical CHF was described earlier and includes oxygen, diuretics, nitroglycerin, and pleurocentesis if necessary. Place the ferret in an oxygen-rich environment and give furosemide at 1 to 4 mg/kg IV or IM. Take a thoracic radiograph after the animal is assessed as being stable and the degree of pleural effusion is determined. The venodilator nitroglycerin reduces pulmonary edema in the acute management of CHF.37 The ointment can be placed on a hairless area of skin every 12 to 24 hours. Monitor the response to initial management of heart failure by closely observing the respiratory rate and effort and ausculting lung sounds. An initial database should be obtained, including values for electrolytes, BUN, and creatinine.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


