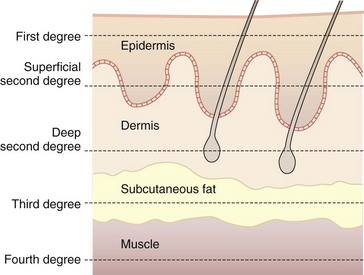
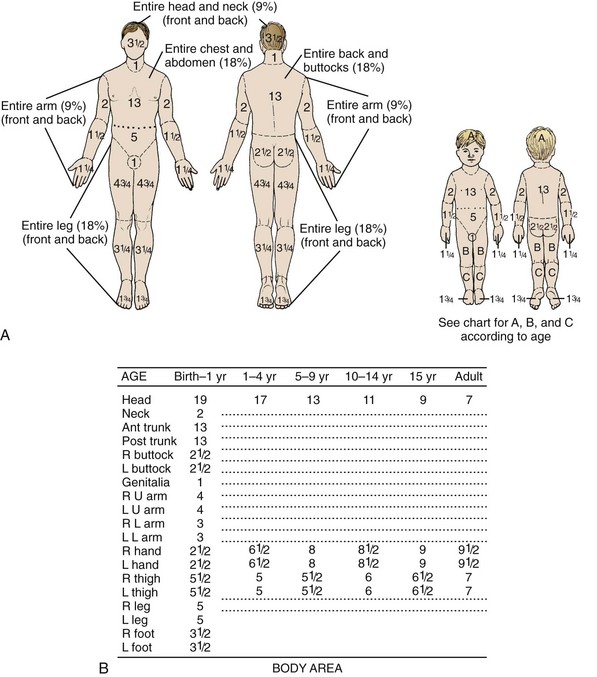
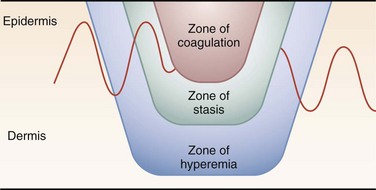
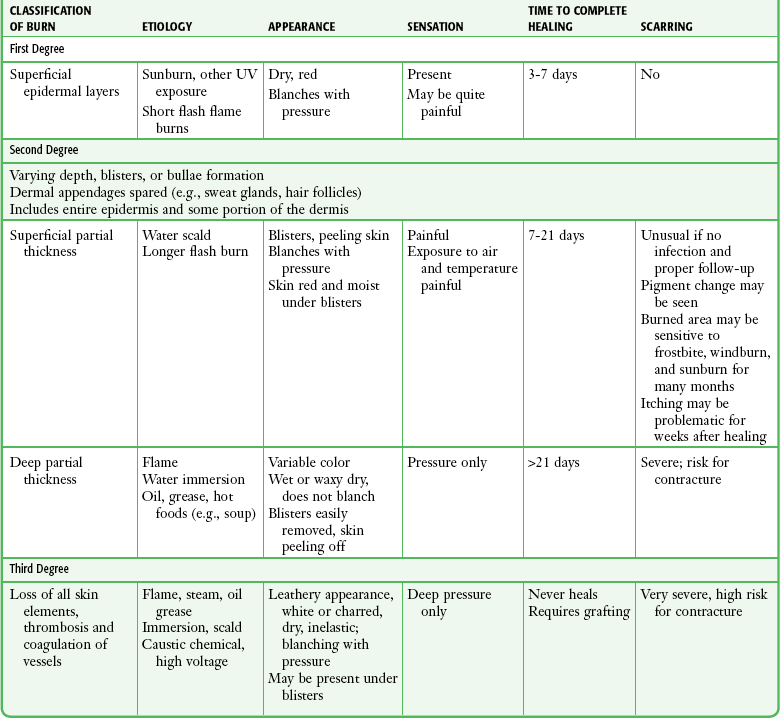
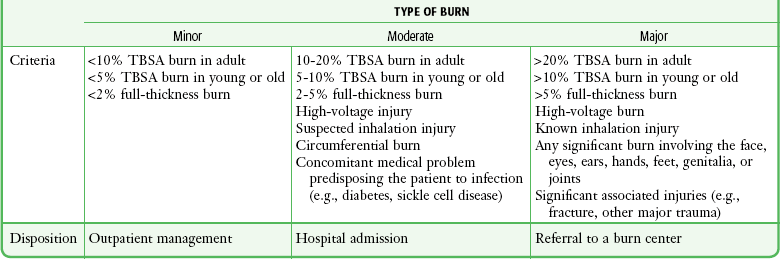
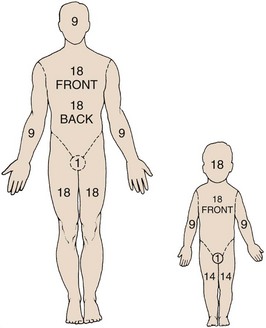
Chapter 38 Two million people suffer a burn-related injury every year in the United States. The American Burn Association (ABA) estimates that approximately 450,000 of these patients received medical evaluation and treatment in 2011 and approximately 10% (45,000) required hospitalization.1 Patients who suffer burn injuries are predominately male (70%), and their mean age is 32 years old. Children younger than 5 years account for 18% of burns, and patients older than 60 years account for an additional 12%. Seventy percent of all burns involve less than 10% of the total body surface area (TBSA). Nearly 80% of all burns are caused by flame or fire or by scalds, with scald injury occurring most in children younger than 5 years. The classification of burns is based on three criteria2: depth of skin injury, percentage of TBSA involved, and source of injury (thermal, chemical, electrical, or radiation). The seriousness of a burn injury is determined by the characteristics and temperature of the burning agent, the duration of exposure, the location of the injury, the presence of associated injuries, and the age and general health of the victim (Table 38-1). TABLE 38-1 Characteristics of Burns, by Depth Modified after Clayton MC, Solem LD. No ice, no butter: advice on management of burns for primary care physicians. Postgrad Med. 1995;97:151; and Morgan ED, Bledsoe SC, Barker J. Ambulatory management of burns. Am Fam Physician. 2000;62:2015. The ABA defines minor burns as uncomplicated partial-thickness burns involving less than 5% TBSA in children (<10 years old) or the elderly (>50 years old), less than 10% TBSA in adults, or full-thickness burns less than 2% TBSA.3 Moderate or major burns include injuries that involve a greater TBSA, as well as burns in areas of specialized function, such as the face, hands, feet, and perineum. More serious burns also include those caused by a high-voltage electrical injury or those with associated inhalation injuries or other major trauma. Emergency clinicians should be aware that the depth of a burn wound cannot always be determined accurately on clinical grounds alone at initial evaluation and that burn injury is a dynamic process that may change over time, particularly during the 24 to 48 hours after the burning process has been arrested. It is common, for example, for a seemingly minor or superficial burn to appear deeper on the second or third return visit (Fig. 38-1). This phenomenon is not a continuation of the burning process that can be altered by clinician intervention but is considered to be a pathophysiologic event related to tissue edema, dermal ischemia, or desiccation.4 The depth of a burn is commonly classified by degree.5 First degree involves the epidermis only, second-degree (or partial-thickness) burns extend into the dermis, and third-degree (or full-thickness) burns destroy the entire skin. An additional fourth degree is sometimes used to describe injuries to the underlying muscle, tendon, or bone (Fig. 38-2). First-degree burns involve the epidermis only (Fig. 38-3A). The skin is reddened but is intact and not blistered. This injury ranges from mildly irritating or even pruritic to exquisitely painful. Minor edema may be noted. Causes include ultraviolet light (as in sunburn) and brief thermal “flash” burns. First-degree burns may blister within 24 to 36 hours, and the patient should be warned about this possibility. Frequently, the epidermis flakes or peels within 5 to 10 days. Healing occurs spontaneously, usually without scarring. Second-degree burns involve the epidermis and extend into the dermis to include the sweat glands and hair follicles. Superficial second-degree burns involve only the papillary dermis (see Fig. 38-3B). These burns are pink, moist, and extremely painful. Blisters are common and the skin may slough. The burn blanches with pressure, and mild to moderate edema is common. Hair follicles are often intact. Superficial second-degree burns are the most common burns seen in the emergency department (ED). The usual causes are scalds, contact with hot objects, or exposure to chemicals. Barring infection or repeated trauma, these burns heal spontaneously and without scarring in about 2 weeks. These areas may be sensitive to sunburn, windburn, and skin irritation for months after the original injury has healed. Deep second-degree burns involve the reticular dermis and appear mottled white or pink (see Fig. 38-3C). There is obvious edema and sloughing of the skin, and any blisters are usually ruptured. Blanching is absent. These burns are not generally painful initially and may have decreased sensation, but pressure may be perceived. Within a few days, however, these burns can become exquisitely painful. This type of burn may be converted to a full-thickness injury by further trauma or infection. Third-degree burns result from complete loss of the dermis and may extend into subcutaneous (SQ) tissue (see Fig. 38-3D). These burns usually appear dry, pearly white, or charred. They are initially painless, with a leathery texture. Circumferential third-degree burns on an extremity or the torso cause a loss of elasticity that may impair the circulation or ventilation and necessitate an escharotomy. Fourth-degree burns extend deeply into SQ tissue, muscle, fascia, or bone (see Fig. 38-3E). These burns are characteristically caused by contact with molten metal, flame, or high-voltage electricity. A more practical method of classifying burns is to describe them as either superficial or deep because this approach defines both treatment and prognosis. Superficial burns involve the papillary dermis, with its rich vascular plexus, and the epidermis, which permits spontaneous healing by reepithelialization from the dermal appendages, including hair follicles, sebaceous glands, and sweat glands. This usually occurs within 2 weeks with minimal scarring. Superficial burns appear wet, pink, and blistered and blanch with pressure. They are painful. Deep burns involve the reticular dermis and SQ fat and generally lack sufficient epithelial appendages for spontaneous healing. If healing does occur, it will occur slowly and produce unstable skin, hypertrophic scarring, and contracture. Deep burns are best treated by excision and skin grafting. The initial appearance of deep burns ranges from cherry red, mottled, white, and nonblanching to leathery, charred, brown, and insensate (Table 38-2). TABLE 38-2 American Burn Association’s Grading System for Burn Severity and Disposition of Patients* TBSA, total body surface area (percentage) affected by the injury. *Burn, partial-thickness or full-thickness burn, unless specified; young, patient younger than 10 years; adult, patient 10 to 50 years of age; old, patient older than 50 years. Adapted with permission from hospital and prehospital resources for optimal care of patients with burn injury: Guidelines for development and operation of burn centers. American Burn Association. J Burn Care Rehabil. 1990;11:98; with additional information from Hartford CE. Care of outpatient burns. In: Herndon DN, ed. Total Burn Care. Philadelphia: Saunders; 1996:71. Although bedside evaluation of very superficial or deep wounds presents little diagnostic difficulty, clinical assessment of a mid-dermal or “indeterminate” burn is accurate only about two thirds of the time.6 Even though it is useful to initially characterize the extent of the burn, it must be noted that the early appearance of a burn wound may not accurately reflect the true extent of the soft tissue injury. Reexamination and follow-up are critical because burn wounds may change during the 24 to 72 hours following injury. Indeterminate burns may eventually heal spontaneously, or they may convert to deeper wounds requiring excision and skin grafting (see Fig. 38-1). Estimating burn size assists practitioners in determining the initial fluid requirements and prognosis. Several formulas are available to estimate TBSA in burn patients. In 1944, Lund and Browder published the now famous Lund-Browder chart (Fig. 38-4).7,8 In their landmark paper, they used direct measurements and body surface area formulas to produce a chart that clinicians can use to estimate %TBSA. The initial Lund-Browder chart was developed from human anatomic studies derived from 11 adults (3 women and 8 men) and produced a unisex chart. A more recent study involving 60 volunteers determined that the Lund-Browder chart significantly underestimates the size of chest burns in large-breasted women. The investigators developed a table that incorporates a correction using brassiere cup size.9 The simplest method for estimating TBSA in adults is the “rule of nines.” This formula was developed in the late 1940s by Pulaski and Tennison, who observed that the percentage of each body segment was approximately a multiple of nine (Fig. 38-5).10 Similar formulas for children adjust estimates for their disproportionately large head surface area. Figure 38-5 The “rule of nines.” The rule of nines is a rough estimate of the total body surface area (TBSA) burned. Note that adults and children are different. This formula frequently overestimates the extent of a burn in clinical practice. As a rough guide, the area covered by the individual’s palm is approximately 1.25% TBSA. See Figure 38-4 for a more accurate method of determining TBSA burned in children. The size of a burn can also be estimated by using the patient’s hand as representing approximately 1% TBSA. With this method, the hand is a rectangle. However, two studies using planimetry have determined that the hand actually represents from 0.5% to 0.78% of a patient’s TBSA.11 One thermal wound theory describes three zones of injury in burns (Fig. 38-6)12: 1. Zone of coagulation: dead, avascular tissue that must be débrided. 2. Zone of stasis: injured tissue in which blood flow is impaired. Desiccation, infection, or mechanical trauma may lead to cell death. 3. Zone of hyperemia: minimally injured, inflamed tissue that forms the border of the wound. The hyperemia usually resolves within 7 to 10 days but may be mistaken for cellulitis. Histologically, full-thickness burns are characterized by confluent vascular thrombosis involving arterioles, venules, and capillaries. Edema secondary to loss of microvascular integrity results not only from the effects of direct thermal injury but also from the release of vasoactive mediators. The increase in vascular permeability is linked to activation of complement and release of histamine. Histamine increases catalytic activity of the enzyme xanthine oxidase, with resultant production of hydrogen peroxide and hydroxyl radicals. These by-products increase the damage to dermal vascular endothelial cells and result in progressive vascular permeability.13 One of the first steps in minor burn care is to select patients for whom outpatient care is appropriate. For patients determined to require inpatient care, the admit or transfer decision depends on the burn care capabilities of the initial treating facility. Guidelines set forth by the ABA14 regarding criteria for referral to a burn center are listed below. Burn injuries that should be referred to a burn center include the following: 1. Partial thickness burns greater than 10% TBSA 2. Burns involving the face, hands, feet, genitalia, perineum, or major joints 3. Third-degree burns in any age group 4. Electrical burns, including lightning injury 7. Burn injury in patients with preexisting medical disorders that could complicate management, prolong recovery, or affect mortality 8. Any patient with burns and concomitant trauma in which the burn injury poses the greatest risk for morbidity or mortality after emergency or surgical stabilization of the traumatic injuries 9. Burned children in hospitals without qualified personnel or equipment for the care of children 10. Burn injury in patients who will require special social, emotional, or rehabilitative intervention Poor candidates for outpatient care of even minor burns include patients with concomitant medical problems such as diabetes mellitus, peripheral vascular disease, congestive heart failure, and end-stage renal disease; patients taking steroids or other immunosuppressive agents; patients who are very young or very old; those who are mentally impaired or have drug and alcohol dependency; homeless persons; those who are malnourished; and patients without a sufficient home support system. Inpatient treatment should be considered in these circumstances even though the burn might be considered “minor” by ABA criteria. Other admission considerations include pain control, the ability to return for follow-up care, the degree of incapacity, the ability to receive wound care at home, and the overall social situation—all should influence the final decision of whether admission is warranted.15 1. Patients requiring intravenous (IV) access. Following a burn there is an immediate capillary leak of plasma-like fluid that can last for 18 to 24 hours. In burns involving greater than 20% TBSA, the leak occurs in both burned and nonburned tissues. If not replaced, this fluid loss can lead to hypovolemic shock and renal failure. IV fluid resuscitation is indicated for all patients with second- and third-degree burns greater than 10% TBSA, in patients younger than 10 or older than 50 years, and for burns greater than 20% TBSA in all other age groups. 2. Anticipated surgery. Deep burns are best treated by early surgical excision and skin grafting. This permits faster wound healing, provides more stable skin, and reduces contractures. Hospital admission facilitates wound care and preparation for surgery. 3. Respiratory problems. Patients with respiratory distress requiring oxygen therapy and those suspected of inhaling toxic fumes or vapors should be admitted for observation or intubation and mechanical ventilation (Box 38-1). Direct bronchoscopic evaluation of the airway may assist in the evaluation and diagnosis of tracheobronchitis or pneumonitis from a smoke inhalation injury. 4. Need for special nursing care. Specialized wound care, dressings, and nursing care are often required for burns involving the face, hands, feet, perineum, and genitalia and are best treated on an inpatient basis. Patients unable to care for themselves or those lacking family and friends able to assist them may also require admission. 5. Special burn injuries. Chemical injuries are often more severe than the initial examination would suggest. Unlike thermal burns, tissue destruction may continue many hours after injury. Patients with chemical injuries should be admitted whenever the injuries are of indeterminate depth, affect a large area, or are deep and require surgical excision or if there are systemic manifestations of chemical toxicity or when the chemical responsible for injury requires a specific antidote. Swelling from deep circumferential burns may constrict the chest or limbs and result in compartment syndrome. Such burns should monitored frequently to determine the need for escharotomy or fasciotomy (Fig. 38-7). Whenever the patient’s condition prevents a reliable clinical examination, direct measurement of compartment pressures can provide an objective measurement of intracompartmental pressure and assist in the decision to perform these surgical procedures (see Chapter 54). Patients with extensive burn injuries that require fluid resuscitation with large volumes of crystalloid should be monitored closely for the development abdominal compartment syndrome. Patients with mechanical burns involving large areas of skin loss and with significant frostbite injuries are generally admitted for specialized wound care and parenteral pain management. Patients with electrical injuries are often admitted for cardiac monitoring, specialized wound care, or both. Cooling is most beneficial for small burns if started within 3 minutes of injury and possibly of additional benefit if continued for the first few hours after the burn. Doing so has been shown to reduce pain significantly and can limit tissue damage by decreasing thromboxane production. When cooling a burn wound, it is important to avoid hypothermia or freezing of tissue because this may deepen the injury.16 At home or in the field, room-temperature or cold tap water irrigation, immersion, or compresses (20°C to 25°C) will provide some pain relief without the risk of further injuring burned tissues and inducing hypothermia, which can occur with iced solutions (Fig. 38-8).17,18 Placing ice on a burn should not be done. Sterile dressings are not required for field treatment; a moist towel or nonadherent sheet may be used. Nonmentholated shaving cream makes an excellent temporary covering for out-of-hospital use if a dressing is not available.19 Home remedies, such as butter or Vaseline, are best avoided but are probably benign.20 Remove jewelry and gross debris in the field if possible. Major burns require the specialized resources of a burn center. Emergency physicians should initiate the resuscitation, consult the burn center for referral, and transfer the patient as soon as practically possible. Initial resuscitation should follow standardized trauma protocols, including a primary and secondary survey, and provide immediate interventions directed at airway management, breathing, and cardiovascular support, as needed. IV catheters can be inserted initially through burned skin when unburned sites are unavailable. Early IV access permits the administration of resuscitative fluids, medications, and parenteral narcotics to relieve the pain. Patients with burns exceeding 20% TBSA should receive IV fluid resuscitation with lactated Ringer’s solution based on the Parkland or Brooke formulas (Box 38-2). More recently, the U.S. Army Institute of Surgical Research has advocated a simpler formula for estimating hourly fluid requirements in burn patients. This simpler formula may be more useful for prehospital providers or ED resuscitation (Box 38-3). The formulas estimate hourly fluid requirements and must be adjusted up or down to achieve a urine output of 0.5 to 1.0 mL/hr. Insertion of a Foley catheter is usually necessary to accurately measure hourly urine output. Patients exposed to carbon monoxide should have carboxyhemoglobin levels measured and empirically receive 100% oxygen for 6 hours. Once considered a traditional empirical treatment, there is no evidence-based proven benefit from hyperbaric oxygen therapy for carbon monoxide poisoning. A recent Cochrane review (http://summaries.cochrane.org/CD002042) concluded that there is insufficient evidence to support the use of hyperbaric oxygen for the treatment of patients with carbon monoxide poisoning. The Cochrane review of published trials found conflicting, potentially biased, and generally weak evidence regarding the usefulness of hyperbaric oxygen for the prevention of neurologic injury. Per an evidence-based analysis, existing randomized trials do not establish whether the administration of hyperbaric oxygen to patients with carbon monoxide poisoning reduces the incidence of adverse neurologic outcomes. Because there may still be advocates of hyperbaric oxygen therapy, consultation with a local hyperbaric center is reasonable, but it is not standard that this intervention be routinely implemented. Critically ill and pregnant patients are still often offered hyperbaric treatment, but controversy over the efficacy and safety persists even for these subgroups. Prompt cooling of the burned part is an almost instinctive response and is one of the oldest recorded burn treatments, having been recommended by Galen (ad 129-199) and Rhazes (ad 852-923).4 In the ED, room-temperature or cold tap water irrigation, immersion, or compresses (20°C to 25°C) are optimal in obtaining pain relief and providing some measure of protection for burned tissues without the problems of hypothermia that iced solutions can cause.8,9 If not done before ED treatment, immediate cold water immersion may still have some ability to limit the extent of a burn and will provide significant pain relief. It is acceptable to add a few ice chips to the water, but packing the wound in ice must be avoided. All involved clothing and jewelry (such as rings), along with any gross debris, should be removed from the burned area. Chemical burns involving the skin or eyes require prolonged tap water irrigation. The burn should otherwise be covered with a moist, sterile dressing. In the ED and prehospital phase, appropriate analgesics, usually narcotics, are the best way to control pain and should not be forgotten in the initial phase of burn care. The burned area may be immersed immediately in room-temperature water or covered with gauze pads soaked in room-temperature water or saline (see Fig. 38-8). The gauze may be kept cool and moist to provide continued pain relief; the patient will let the clinician know when additional cooling is desired. Many clinicians use sterile saline for cooling, but it has no proven benefit over tap water, even when the skin is broken. It is acceptable to add ice chips to water or saline to lower the temperature. As stated previously, immersion of burned tissue in ice or ice water should be avoided because ice immersion increases pain and risks frostbite injury or systemic hypothermia. The potential benefits of burn cooling are listed in Box 38-4. Because most patients with minor burns seek medical attention after initial self-instituted prehospital cooling, it is unlikely that the clinician can favorably affect the burned tissue with any intervention in the ED. With the exception of pain relief and removal of debris, the primary benefits of burn cooling are probably experienced only if the burn is cooled promptly, within the first 3 minutes after injury, thus making home care important.21,22 Minor burns are considered tetanus prone, and tetanus toxoid should be administered if patients are unsure of their tetanus immunization status or when it has been more than 10 years since the last immunization. Nonimmunized patients should receive human tetanus immune globulin, 250 units intramuscularly, along with tetanus toxoid and a booster injection of toxoid in about 3 weeks. Minor burns are generally those that will heal spontaneously and do not require surgery or specialized wound care. These wounds are not associated with immunosuppression or hypermetabolism, nor are they highly susceptible to infection, a quality associated with larger burns.23,24 Treated conservatively, most minor burns will heal without significant scarring. Many complications seen with minor burns are thought to result from overtreatment rather than undertreatment. Examples include the use of dry dressings that can adhere to newly forming skin and secondary infections from the overzealous use of topical or systemic antibiotics. The most important characteristic of a dressing is that it controls fluids within the wound. Burn dressings that keep the surface of the wound moist and avoid pooling of fluids will speed healing.25 The best material for this purpose is a generous amount of simple dry gauze applied over a nonadherent dressing or topical preparation. The outer layer of dressing should be porous to permit evaporation of water from the absorbent dressing material. Some clinicians prefer to eschew a nonadherent portion of the dressing so that subsequent dressing removal aids in minor débridement. Wound preparation and basic bandaging should include the following steps (Fig. 38-9): 1. Cleanse the burned area gently with a clean cloth or gauze and a mild antibacterial wound cleaner such as chlorhexidine, and irrigate the wound with saline or water. It is not necessary to shave the hair in or around the wound. There is no benefit to vigorously washing a minor wound with strong antiseptic preparations (such as povidone-iodine [Betadine] and others).24 2. Débride blisters and sloughed skin initially by peeling the devitalized skin from the wound (Fig. 38-10A-C). Blisters can be opened with scissors and forceps. If necessary, analgesia should be provided for any painful débridement. The initial débridement should attempt to remove only grossly devitalized tissue. Additional débridement of the wound can take place, if needed, during subsequent follow-up visits when the wound has matured. 3. Consider applying a layer of antibiotic cream or ointment such as 1% silver sulfadiazine (Silvadene) or bacitracin directly to the wound (see Fig. 38-10D). 4. Apply fine-mesh gauze or commercial nonadherent gauze such as Adaptic or petrolatum gauze impregnated with 3% bismuth tribromophenate (Xeroform) to the burn wound. 5. Cover and pad the wound with loose gauze fluffs. If fingers and toes are involved, pad the web spaces and the digits individually and separate them with strips of gauze (see Fig. 38-9D and 38-10E and F). The entire dressing is wrapped snugly (but not tightly) with an absorbent, slightly elastic material such as Kerlix. 6. The patient should be instructed to elevated the affected limb to prevent swelling, which may cause delayed burn conversion or wound infection. Biologic Dressings: Biologic dressings are natural tissues, including skin, that consist of collagen sheets containing elastin and lipid. They are not routinely used in the emergency care of minor wounds. The benefits of biologic dressings include a reduction in surface bacterial colonization, diminished fluid and heat loss, avoidance of further wound contamination, and prevention of damage to newly developed granulation tissue. Examples of biologic dressings include cadaveric human skin and commercially available porcine xenograft or collagen sheets. Synthetic Dressings: Synthetic dressings are manufactured in various forms. Film-type dressings have a homogeneous structure and are usually polymers. Because these dressings are nonpermeable, problems with retention of wound exudates have occurred. Some second-generation dressings have been developed to address these problems. These products include Tegaderm, Vigilon, DuoDERM, Biobrane, Op-Site, Omniderm, and Sildimac.25,26 These preparations have theoretical benefits under certain circumstances, but none has proved to have superior performance over simple gauze dressings for minor outpatient burns. These products are most often used by burn centers and have little applicability for minor burns in patients discharged from the ED. For patients admitted or transferred to a burn center, simple gauze dressings are appropriate. Some burn centers prefer that topical agents not be applied before transfer so that the full extent of the burn can be assessed immediately. Analgesia: Pain is a critical feature of any burn injury. Relief of pain by the appropriate and judicious use of narcotic analgesics is of the utmost importance in the initial care of all burn patients. Prehospital narcotics are very appropriate when standard contraindications do not exist. Analgesia should be provided before extensive examination or débridement is performed. Inadequate analgesia is probably the most common ED error in the treatment of burn injuries, especially when burns occur in children. Parenteral narcotic analgesics have been erroneously relegated to pain control only for major burns, but it is suggested that narcotics be generously administered in the initial treatment of even minor painful burns. Parenteral opioids (fentanyl, 1 to 2 µg/kg, or morphine, 0.1 to 0.2 mg/kg) are usually required, especially if painful procedures such as débridement and dressing changes are planned. We prefer to use IV opioids (occasionally supplemented with a short-acting benzodiazepine such as midazolam) for all painful procedures. For complicated débridement or dressing changes, adequate analgesia and sedation (see Chapter 33) is strongly advocated. Pruritus: Postburn pruritus is one of the most common and distressing complications of burn injury and is estimated to affect 87% of burns.27 It typically develops in the subacute phase and is therefore not a common issue for the emergency clinician in the acute treatment phase. Despite the limited literature on the treatment of postburn pruritus, available therapies include oral antihistamines, topical antihistamines, and topical moisturizers. The use of topical therapies should be withheld until sufficient wound healing has occurred. Edema: Minor burns lead to immediate inflammation mediated by the release of histamine and bradykinins, which cause localized derangements in vascular permeability with resultant burn wound edema. This edema may be harmful in several ways. First, the increase in interstitial fluid increases the diffusion distance of oxygen from capillaries to cells and thereby increases hypoxia in an already ischemic wound. Second, the edema may produce untoward hemodynamic effects by a purely mechanical mechanism: compression of vessels in muscular compartments. Third, edema has been associated with the inactivation of streptococcicidal skin fatty acids, thus predisposing the patient to burn cellulitis.28,29 Successful management of burn edema hinges on immobilization and elevation. Most patients are unfamiliar with the medical definition of elevation and are not aware or convinced of its value. Patient education in this regard is critical; however, certain burns (e.g., burns in dependent body areas) are prone to edema despite everyone’s best intentions. It is for this reason that lower extremity burns in general and foot burns in particular are prone to problems. Major burns of the hand should be elevated while the patient is still in the ED. This is most readily accomplished by hanging the injured hand from an IV pole with a stockinette to support the bandaged hand (Fig. 38-11). Use of Topical Preparations and Antimicrobials: Minor burns result in insignificant impairment of normal host immunologic defenses, and burn wound infection is not usually a significant problem. Topical antimicrobials are often used; however, some believe that these agents may actually impair wound healing.29 Although the procedure is of unproven value, many clinicians routinely use antibiotic creams or ointments on even the most minor burns. Most patients expect some type of topical concoction, so a discussion of their use—or nonuse—is prudent.
Burn Care Procedures
Wound Evaluation
Estimating Burn Depth
Estimating Burn Size
Histopathology of Burns
Outpatient Versus Inpatient Care
Procedure
Initial Care of Major Burns
Initial Care of Minor Burns
Outpatient Care of Minor Burns
Burn Dressings
Specific Clinical Issues in Minor Burn Care
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Burn Care Procedures