25 Alteration in pupil function
CASE WORK-UP
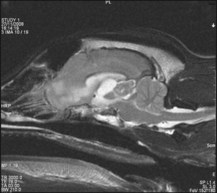
MRI found a contrast-enhancing lesion which was isointense on T1 and of variable intensity on T2WI. There was secondary dilation of the third and lateral ventricles (Fig. 25.1). Within the third ventricle choroid plexus papilloma (CPP) and ependymoma are intraventricular in location and enhance uniformly. Meningiomas can be intraaxial.
CASE HISTORY
The dog had been lethargic for 1 week, lagging behind on exercise and lacking interest on a walk. He had vomited twice. Two days prior to referral, bilateral protrusion of the third eyelids occurred, followed the next day by squinting in the light and bilateral dry nasal discharge. The dog appeared to be urinating more often but was not polydipsic.
CLINICAL EXAMINATION
Gait, posture, proprioception, hopping and spinal reflexes were all normal.
The Schirmer Tear Test (STT) was 0 mm bilaterally.



