The Scapula and Shoulder Joint
 . Approach to the Body, Spine, and Acromion Process of the Scapula
. Approach to the Body, Spine, and Acromion Process of the Scapula
 . Approach to the Craniolateral Region of the Shoulder Joint
. Approach to the Craniolateral Region of the Shoulder Joint
 . Approach to the Craniolateral Region of the Shoulder Joint by Tenotomy of the Infraspinatus Muscle
. Approach to the Craniolateral Region of the Shoulder Joint by Tenotomy of the Infraspinatus Muscle
 . Approach to the Caudolateral Region of the Shoulder Joint
. Approach to the Caudolateral Region of the Shoulder Joint
 . Approach to the Caudal Region of the Shoulder Joint
. Approach to the Caudal Region of the Shoulder Joint
 . Approach to the Craniomedial Region of the Shoulder Joint
. Approach to the Craniomedial Region of the Shoulder Joint
 . Approach to the Medial Region of the Shoulder Joint
. Approach to the Medial Region of the Shoulder Joint
 . Approach to the Cranial Region of the Shoulder Joint
. Approach to the Cranial Region of the Shoulder JointApproach to the Body, Spine, and Acromion Process of the Scapula
Based on a Procedure of Alexander1
Description of the Procedure
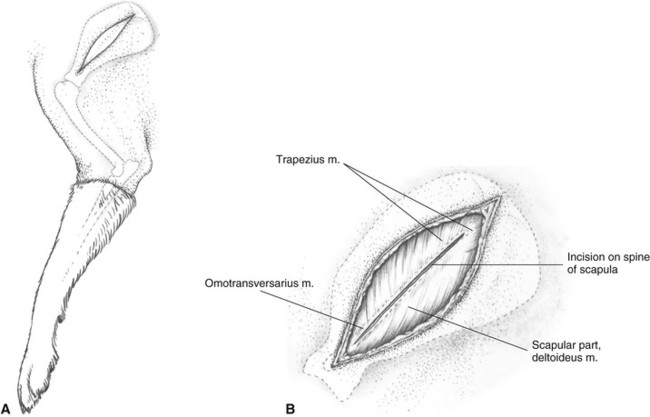
A Identify the spine of the scapula, acromion process, and greater tubercle of the humerus by palpation. The skin and subcutaneous fascial incision is made directly on the spine of the scapula. The skin and fascia are retracted following the undermining of the edges of the incision. The length of the incision is adjusted to fit the area of interest in the exposure.
B An incision is now made in the deep fascia along the spine of the scapula and is deepened to free the origin of the scapular part of the deltoideus and the insertions of the omotransversarius and trapezius muscles. These muscles are freed and retracted sufficiently to expose the spine of the scapula and underlying spinatus muscles.
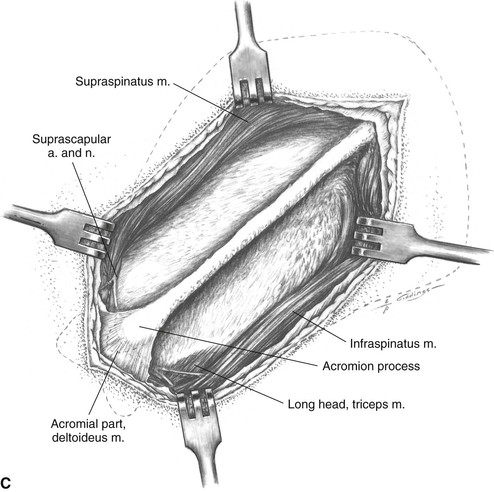
C The infraspinatus and supraspinatus muscles are elevated from the spine of the scapula. The bellies of the muscles can then be bluntly undermined in a distal to proximal direction using a periosteal elevator (see Figure 19) and then retracted from the body of the scapula. Near the acromion, an incision can be made a short distance into the septum between the acromial and scapular parts of the deltoideus to allow retraction of the scapular part (see Plate 28B, C, D).
Additional Exposure
Distal extension to the craniolateral region of the shoulder joint (see Plate 26).
Distal extension to the craniomedial region of the shoulder joint (see Plates 30 and 32).
Precautions
Distally the exposure of the neck of the scapula is complicated by the suprascapular nerve and artery. The suprascapular nerve emerges around the scapular notch, supplying a branch to the overlying supraspinatus muscle. The nerve then crosses the neck of the scapula distal to the scapular spine to supply the infraspinatus muscle.
Approach to the Craniolateral Region of the Shoulder Joint
Alternative Approaches
The exposure provided by this craniolateral approach (see Plate 26) is generally much greater than is needed for osteochondritis dissecans surgery. It is only recommended when the surgeon has no assistant to retract and position the limb, as is needed for the other recommended approaches (see Plates 27, 28, and 29).
Description of the Procedure
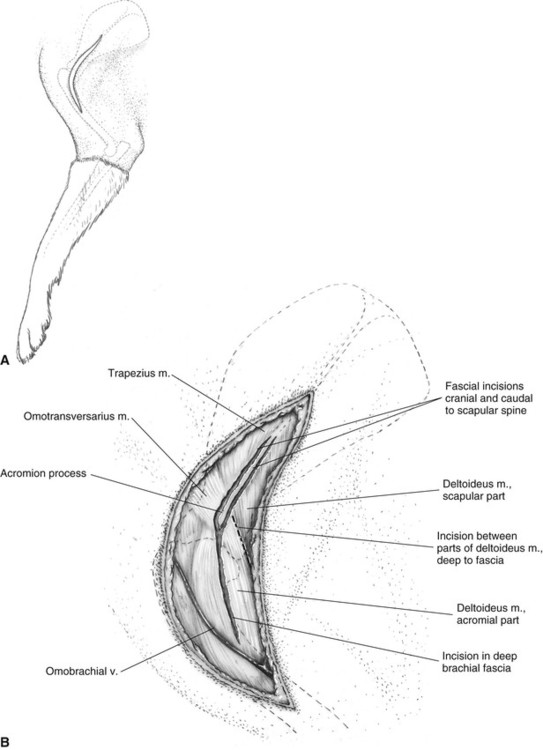
A Identify the spine of the scapula, acromion process, and greater tubercle by palpation. The curved incision begins at the middle of the scapula and follows the spine distally, crossing the joint and continuing over the lateral surface of the humerus to the midpoint of the shaft. The skin margins are undermined and retracted after the subcutaneous fascia and fat are incised in the same line as the skin incision.
B An incision is made in the deep fascia, starting distally at the omobrachial vein and centered over the belly of the acromial part of the deltoideus. It continues proximally toward the acromial process, passing through the craniodistal insertion of the omotransversarius muscle, and onto the spine of the scapula. The scapular incision encompasses the distal one third of the spine and is deepened both cranial and caudal to the spine to include the insertions. Protect the branches of the axillary nerve entering the deep surface of the deltoideus muscle as it is retracted distally of the omotransversarius and trapezius and the origin of the scapular part of the deltoideus muscle. Take care not to incise the underlying spinatus muscles.
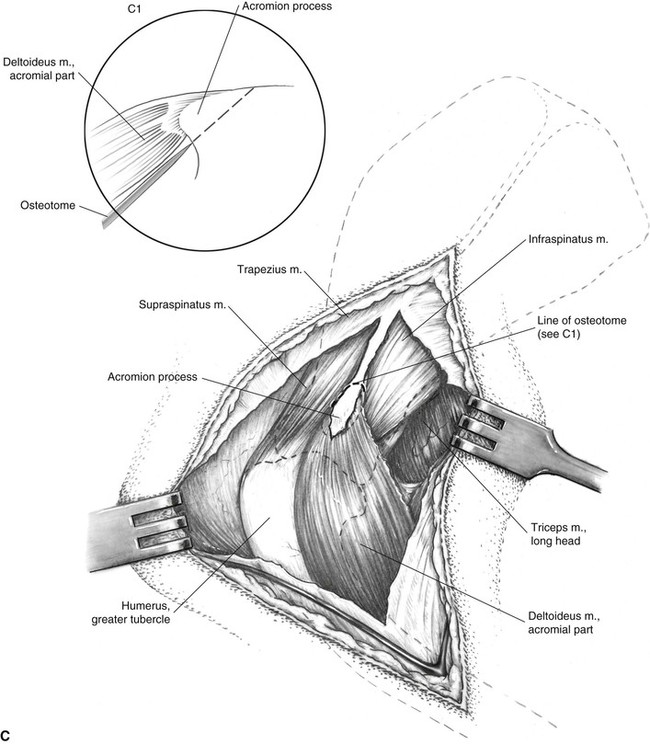
C The omotransversarius and trapezius muscles are retracted craniodorsally. An incision is made between the two parts of the deltoideus muscle (shown in Plate 26B) and is developed bluntly to allow freeing of the scapular part of the deltoideus and its caudoventral retraction. Use care during this dissection to preserve as many as possible of the muscular branches of the axillary nerve that will be found in this area. The area of the acromion is cleared of adherent tissue to allow an osteotomy (see Plate 26C1 for detail). Using a small curved hemostat, separate between the acromial part of the deltoideus muscle and the underlying infraspinatus and supraspinatus muscles, while staying close to the acromion.
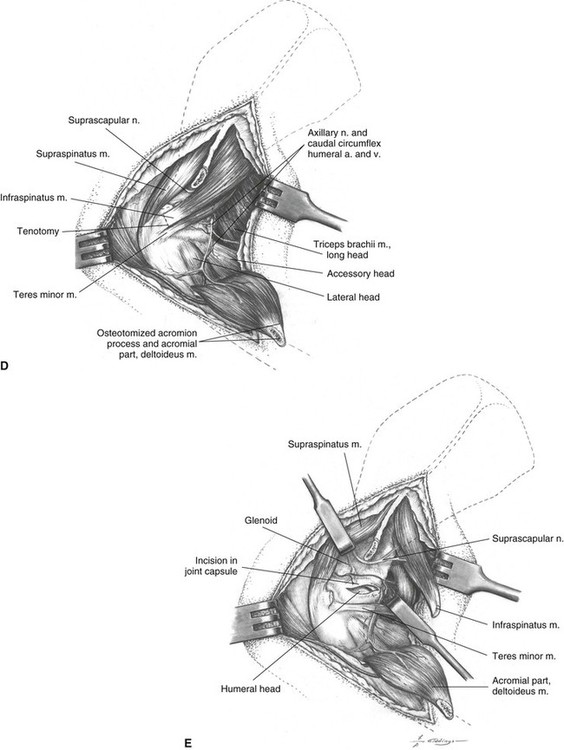
D The acromion is osteotomized to include all of the origin of the acromial part of the deltoideus (see Plate 26C1 for detail). Either an osteotome or a bone-cutting forceps can be used for the osteotomy; in either case, care must be used to protect the underlying suprascapular nerve. Protect the branches of the axillary nerve entering the deep surface of the deltoideus muscle as it is retracted distally. Some surgeons prefer tenotomy of the origin of the deltoideus near the acromion. In young animals the acromion may not be ossified. In these cases, a tenotomy of the acromial part of the deltoideus is performed close to the acromion. Tenotomy is also more satisfactory in small dogs and cats. Holes drilled in the acromion allow for reattachment of the tendon (see Figure 22).
E The supraspinatus and infraspinatus muscles are bluntly elevated from the spine and body of the scapula sufficiently to allow their retraction as shown. Note the position of the suprascapular nerve and avoid this structure during the elevation and retraction of the infraspinatus.
Additional Exposure
Proximal extension to the body and spine of the scapula (see Plate 25).
Extension of the approach to the cranial region of the shoulder joint with osteotomy of the greater tubercle of the humerus provides total exposure of the scapular neck and most of the glenoid cavity (see Plate 32).
Closure
A modified Bunnell-Mayer or locking-loop suture (Figure 21A, C), reinforced with one or two mattress sutures, is used to join the transected infraspinatus muscle. The acromion is attached to the spine by two 20- to 22-gauge monofilament stainless steel sutures placed through holes drilled in the bones (Figure 24B). Several sutures are placed between the two parts of the deltoideus muscle. A single tier of sutures may be used to close the remaining muscles and deep fascia. Starting at the proximal end of the incision the suture engages the deep fascia, the trapezius, the scapular part of the deltoideus, and the deep fascia. This pattern is continued distally, with the omotransversarius replacing the trapezius as the acromion is approached. Distal to the acromion, the deep fascia alone is closed.
Precautions
The suprascapular nerve emerges around the scapular notch, supplying a branch to the overlying supraspinatus muscle. The nerve then crosses the neck of the scapula, distal to the scapular spine, to supply the infraspinatus muscle. The axillary nerve curves around the caudal border of the subscapularis muscle and neck of the scapula, and then it crosses the caudal aspect of the shoulder joint between the joint capsule and long head of the triceps muscle.
Approach to the Craniolateral Region of the Shoulder Joint by Tenotomy of the Infraspinatus Muscle
Based on a Procedure of Hohn20
Alternative Approaches
An alternative is the approach to the craniolateral region of the shoulder with osteotomy of the acromion process (see Plate 26), but it provides more exposure than generally needed for surgical correction of osteochondritis dissecans or infraspinatus contracture and may unnecessarily produce greater surgical trauma.
This craniolateral approach (see Plate 27) gives good exposure to the articular surface of the humeral head, but poorer access to the caudal compartment of the joint for removal of joint mice, compared to the caudolateral (see Plate 28) and caudal (see Plate 29) approaches.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


