39 UMN
Spinal cord infarction
NEUROANATOMICAL LOCALIZATION
The lesion was localized to the cervical spinal cord segments C1–C5, on the right hand side.
CASE WORK-UP
MRI of the cervical cord 4 days after the onset of signs found an area of hyperintensity on T2WI within the right side of the spinal cord at the level of the C4–5 vertebrae. CSF was normal, but this may have reflected sampling rostral to the lesion (Fig. 39.1).
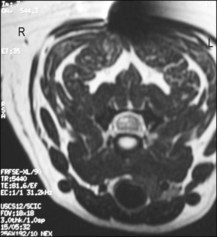
Figure 39.1 Transverse T2WI. Focal hyperintensity within the right side of the cervical spinal cord.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


