Ultrasound
Musculoskeletal
Basic Information 
Preparation: Important Checkpoints
• Patient preparation is very important to minimize artifacts and misdiagnoses.
• Sedation is often necessary to allow proper positioning and expedite the exam. A small amount of sedation is generally sufficient to minimize patient motion; excessive sedation may lead to patient instability.
• Dry dirt and debris within the hair coat can be removed with a firm brush. A mild detergent or scrub can be used to further clean a clipped area.
• The hair coat must be clipped for an optimal image to be acquired. This is because hair and the air trapped between the hair shafts act as an acoustic barrier to the insonating ultrasound beam and the returning echoes.
• Applying 70% alcohol to the clipped area helps reduce small air bubbles remaining in the undercoat.
• Applying an acoustic coupling gel allows optimal transfer of sound waves from the transducer into and out of the patient.
Equipment
• Many different machines are available. These include handheld ultraportable units designed specifically for minor applications to large units mounted on four-wheeled carts designed for stationary use. The majority of equine ultrasound is performed on laptop or portable units.
• The most important aspects of transducer choice are frequency and configuration. Transducers come in several configurations, each having a preferred application.
• Newer transducers are electronic, consisting of multiple (several hundred) small piezoelectric elements, or arrays. The configuration of the piezoelectric crystals is what defines the size, shape, and application of the transducer. Electronic transducers include linear, curvilinear, microconvex, and phased arrays.
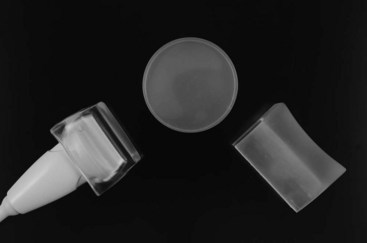
• Linear array transducers are the only suitable choice for equine tendon and ligament examination because of excellent near-field width and high resolution (Figure 1).
• Curvilinear, microconvex, and phased array transducers all produce a form of a sector image (pie shaped).
• Curvilinear transducers have a large radius, a large patient contact area (footprint), and a relatively large near-field view. They are used for deeper areas such as abdominal imaging.
• Microconvex transducers have a very small “tip,” allowing a small area of contact with the patient and producing a sector image with very little usable information in the near field.
• Phased array transducers also produce a sector image and generally have the highest penetration (depth) of any of the transducers. Phased array transducers are the choice for cardiac imaging because high achievable frame rates provide the best visualization of cardiac motion.
• All the sector transducers can be used for evaluating deeper anatomy; musculoskeletal applications include evaluation for deep-seated abscesses and assessing continuity of deeper bony surfaces for fractures.
• Electronic transducer design has many advantages over older mechanical transducer technology, including wide band width (eg, 4–13 MHz) and focusing.
• Wide bandwidth allows the user to preferentially select the frequency range that is most appropriate for the depth of penetration necessary and resolution of image detail. As an example, a linear array transducer capable of operating between 4 and 13 MHz allows visualization of deeper structures at a lower frequency range while very near-field structures can be studied at higher resolution (image detail) using the highest frequency.
• Focusing is a method to increase lateral (side-to-side) resolution with electronic transducers. The focal point (or multiple focal points) provides the best resolution at the selected depth(s). Use of multiple focal points results in a reduction in frame rate (how many times per second the image is updated) which can be bothersome while scanning.
• Older transducers are of the mechanical type, in which a single piezoelectric crystal was oscillated to produce a sector (pie-shaped image), or in some designs consisted of three crystals of different frequencies that rotated to form a sector image. These transducers have a fixed single focus and their frequency cannot be adjusted, except for the annular array design. Mechanical transducers are not available in linear array configuration. These transducers are still operational for imaging deeper areas of the patient such as the heart and abdomen but have little utility today for most extremity tendon and ligament examinations.
• Use the highest frequency transducer available that allows imaging the anatomic area of interest. The higher the frequency of the ultrasound transducer, the better the axial resolution, the trade-off being less penetration of the ultrasound beam. Lower frequency transducers trade less resolution for greater depth of penetration. This is why the broad-bandwidth electronic transducers are so user friendly; one transducer can image a wide range of depth by just varying the available frequency range.
• Most equine musculoskeletal examinations are performed with a high frequency linear transducer, typically from 7.5 to 13 MHz or even 18 MHz. These frequencies allow a usable scanning depth of up to 4 or 5 cm, making them ideal for most tendon and ligament work. A linear probe is used because of its large flat footprint and excellent near-field resolution. The linear configuration emits the ultrasound beam perpendicular to tendon/ligament fibers when properly aimed, in turn yielding the best overall image.
• A standoff pad is made of a flexible, sonolucent material. The purpose of the standoff is to allow better visualization of very superficial structures. Standoff pads may be form-fitted to the transducer or be of a universal application and disposable (see Figure 1). A few newer, dedicated near-field transducers have build-in permanent standoffs. The key to using a standoff pad properly is to ensure adequate acoustic coupling by liberal use of acoustic gel between the transducer and the standoff and the standoff and the patient.
Basic Machine Settings for Obtaining A Quality Image
• Gain controls the brightness of the ultrasound image by uniformly amplifying the returning echoes. The overall gain needed is variable depending on patient preparation, size, skin thickness, etc. The ultrasound image should be bright enough to easily see all structures in the field of view. An entire image that is too dark despite a maximum gain setting is usually due to poor acoustic coupling (hair not clipped, scaly or uneven skin surface, lack of acoustic coupling gel). This emphasizes the importance of achieving the best acoustic coupling of the transducer to the patient as possible. Figure 2 illustrates improper gain settings.
• Increasing the power output of the ultrasound machine can be useful in making an image brighter. The power output is really the volume of the ultrasound being transmitted into the patient. Ultrasound machines are limited in their output by the Food and Drug Administration. The power control may be labeled as P (power) or MI (mechanical index).
• Another common cause of images that are too dark is the presence of high levels of ambient light or reflected light on the monitor. A darkened room is essential. Positioning the patient so that the ultrasound machine is in a shadow may be your only hope to obtain an adequate image in a field setting.
• Time gain compensation (TGC): This is a depth-dependent gain adjustment controlled by a series of sliders or knobs. These controls are set such that the level of image brightness is even from the near field to the far field. In most applications, the near-field gain must be reduced (since near-field echoes are inherently louder because they are not attenuated to the same degree as echoes originating from deeper areas), whereas the far field gain must be boosted. Figure 3 illustrates incorrect TGC settings, rendering the images nondiagnostic. Figure 4 illustrates properly adjusted, diagnostic-quality images.
• When the far field remains too dark despite a maximum overall gain, power setting, and far-field TGC boost, use a lower frequency to obtain adequate penetration.
• The focal zone is the narrowest portion of the ultrasound beam and therefore is the depth of the image that has the best resolution. The focus should be placed at the level of the structure of interest to obtain optimal resolution (see Figure 4). The use of multiple focal zones yields the best image, but the tradeoff is a reduced frame rate, seen as “flicker” when the transducer is moved along its path too quickly.
• There are numerous additional user-defined settings available to adjust the appearance of the ultrasound image. These can be considered fine tuning. An explanation of some of these settings is provided in Figure 4.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


