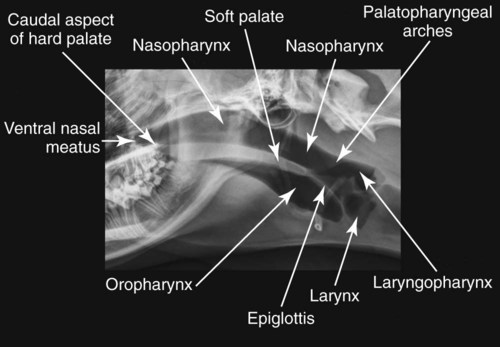
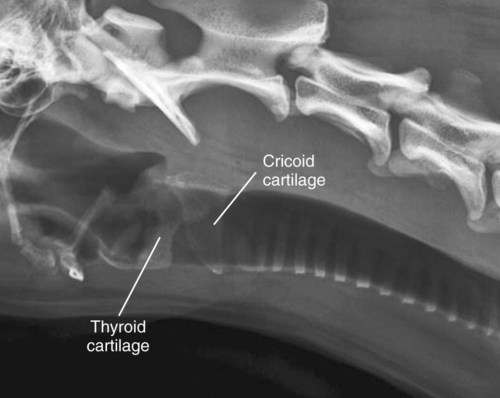
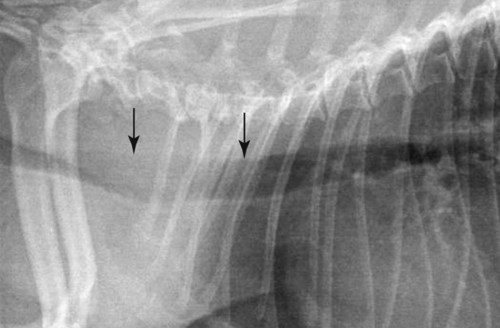
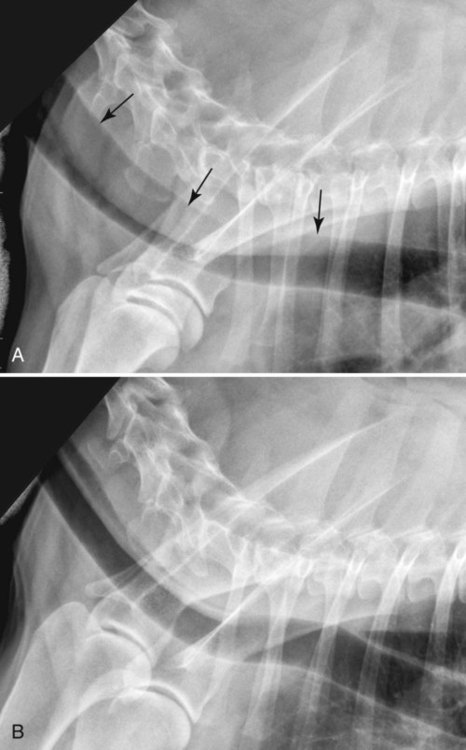
The upper respiratory system comprises the air-filled pharynx, the larynx, and trachea. The pharynx includes the oropharynx ventrally, the nasopharynx dorsally, and larger laryngopharynx caudally. The soft palate divides the oropharynx from the nasopharynx rostrally, and the palatopharyngeal arches, which form the soft tissue line extending caudodorsally from the soft palate, divide the nasopharynx from the laryngopharynx. Finally, the epiglottis divides the oropharynx and laryngopharynx (Fig. 26-1).1 Caudodorsally, the laryngopharynx extends to form the piriform recess. The epiglottis is often surrounded by gas and extends to just overlap dorsally or ventrally the tip of the soft palate.2 In larger dogs, the cuneiform process, which is the rostral portion of the arytenoid cartilage, can be seen occasionally. The other laryngeal cartilages are represented by an indistinct soft tissue opacity superimposed on the laryngeal lumen. Gas-filled ventricular saccules are seen occasionally. In older dogs, and even younger large-breed dogs, laryngeal cartilages become identifiable because of mineralization, the cricoid being the most readily evident (Fig. 26-2).3 Tracheal rings may also mineralize with age and become visible. Typically the pharynx has the widest lumen, followed by the larynx and then trachea, which is mildly smaller in diameter. A ratio between tracheal diameter and thoracic inlet height is proportionally larger in dogs with greater body weight and smaller in brachycephalic breeds.4 Tracheal luminal diameter is similar between the cervical and thoracic regions, but sometimes widens caudally in the cervical region in large-breed dogs. Tracheal diameter can also vary mildly between inspiration and expiration. Variable tracheal luminal narrowing in dogs can be caused by a so-called redundant trachealis dorsalis membrane, between the midcervical and midthoracic portions of the trachea (Video 26-1, Figs. 26-3 and 26-4). The narrowing caused by a redundant dorsal tracheal membrane can be dynamic, depending on phase of respiration (see Fig. 26-4). Other explanations for this appearance are displacement of the esophagus ventrally between the incomplete dorsal aspects of the tracheal rings and tracheal rotation, but a redundant drooping membrane is most common. In most dogs, a redundant dorsal tracheal membrane is not responsible for clinical signs, but it can be confused easily with tracheal collapse. The redundancy can be marked, with the resulting superimposed soft tissue opacity almost completely obscuring the tracheal lumen. Differentiation from tracheal collapse lies in identifying the slightly more opaque dorsal tracheal wall at its normal location when the narrowing is caused by a redundant membrane. The position of the thoracic portion of the trachea can vary with patient positioning. Normally, it is approximately parallel with the spine, although it is slightly closer to the spine through the thoracic inlet. When the patient’s head is ventroflexed, focal dorsal displacement of the trachea can mimic a cranial mediastinal mass (Fig. 26-5). Conversely, extreme extension of the neck can cause tracheal compression. On a dorsoventral radiograph, the thoracic portion of the trachea is located on or curves mildly to the right of midline.5 In brachycephalic breeds and obese dogs with mediastinal widening, the trachea curves more markedly to the right, and this should not be confused with displacement from a mass, such as from a heart base tumor (Fig. 26-6). Indications for radiography of the pharyngolarynx are respiratory difficulty and stertor caused by a suspected upper respiratory obstruction; ptyalism, gagging, and dysphagia; dysphonia; a palpable mass, or a visible draining tract. Although ultrasound is useful for evaluating the soft tissues surrounding the upper respiratory tract, radiography is better for assessing their impact on the upper respiratory tract lumen. In addition, radiography can help screen for nonpalpable masses.6 As for any hollow organ, pharyngolaryngeal masses may be extramural, mural, or intraluminal. Extramural masses can originate from any of the structures surrounding the pharyngolarynx (Box 26-1) and may be neoplastic (Fig. 26-7), infectious (Fig. 26-8), traumatic, hemorrhagic, or other in nature. Radiographically, extramural masses are usually poorly defined from the surrounding soft tissues and appear as areas of soft tissue thickening, which may cause displacement and/or narrowing of the respiratory tract lumen. Their interface with the air-filled lumen is smooth, rounded, and broad-based. Their origin is determined based on their location relative to the pharyngolarynx. In cats, the two most common forms of pharyngolaryngeal mural neoplasia are lymphoma and squamous cell carcinoma, and in the larynx the arytenoid cartilage is most often involved.7,8 In dogs, in the pharynx, squamous cell carcinoma and melanoma are reported;9 in the larynx, epithelial tumors and rhabdomyoma are most frequent, although mast cell tumor, various sarcomas, oncocytoma, and melanoma are also seen (Fig. 26-9).8,10 Mural masses tend to be smaller when clinical signs appear, given that their impact on the respiratory lumen is more direct. As a result, they can be very difficult to identify radiographically, and endoscopy or direct pharyngolaryngoscopic examination may be more useful. Superimposition of the normal laryngeal cartilage can make laryngeal masses difficult to detect. Masses are characterized primarily by an increase in the normal soft tissue opacity, as with diffuse thickening, decreased margination of pharyngolaryngeal structures, and/or airway stenosis (Fig. 26-10).7 They can also appear well defined (Fig. 26-11) and/or lobulated if surrounded by air.8 Horizontal epiglottic displacement can also occur.11 Pharyngolaryngeal trauma occurs most often because of a penetrating wound originating either internally from the upper respiratory tract or esophagus, such as with a stick injury, or externally, such as a bite wound or gunshot. Blunt trauma from choking is another possibility. Soft tissue thickening representing swelling and or a mass may be found with hematoma, cellulitis, myositis, and/or abscess. Gas opacities can be found in the subcutaneous tissues and between muscle and tissue planes. If linear, these represent emphysema, whereas more focal and rounded gas accumulation may indicate abscess (Fig. 26-12). Emphysema has been reported in 83% of dogs with acute oropharyngeal stick injury and can extend to pneumomediastinum, pneumothorax, mediastinitis, and pleural effusion.12 Pharyngeal diverticulum13 and stenosis can be complications of trauma. Brachycephalic syndrome comprises a complex of upper respiratory disorders in brachycephalic breeds of dogs and cats. Diagnosis is typically made by clinical and laryngoscopic examination. Radiographically, elongated soft palate and soft palate edema appear as an extension and thickening of the soft palate beyond the tip of the epiglottis, and subsequent narrowing of the nasopharyngeal and oropharyngeal diameters (Fig. 26-13). Laryngeal collapse can also be present, but because it occurs in a laterolateral direction, it is not seen commonly on radiographs unless the collapse is severe (Fig. 26-14). Tracheal hypoplasia (see trachea section) is diagnosed radiographically.
The Pharynx, Larynx, and Trachea
Anatomic Considerations: Normal Anatomy and Radiographic Technique
Radiographic Signs of Disease
Pharyngolarynx
Masses
Trauma and Foreign Body
Brachycephalic Syndrome
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


The Pharynx, Larynx, and Trachea