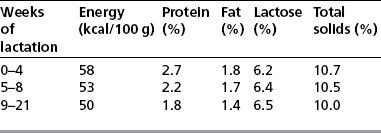
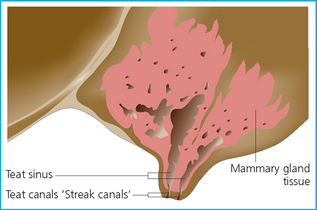
Chapter 10 The mammary gland is a vital part of the reproductive anatomy of the mare. There is no doubt that milk is the ideal food for the very young foal, and under natural conditions continues to provide important nourishment for the growing foal up to natural weaning (often at about 8–9 months of age). Furthermore, the mammary gland plays a vital role in providing early immunological protection for the foal through the production of immunoglobulin-rich colostrum. Without effective production of high-quality colostrum containing appropriate antibody IgG, the foal has a dramatically reduced chance of survival1 (see p. 374). Of all the domestic species, the foal is probably the most reliant upon colostral intake for its survival in the first few weeks of extrauterine life. The mare has two mammary glands separated completely by a facial sheet. There is one teat per gland.2 Each teat usually has two openings (Fig. 10.1), but occasionally there are three, reflecting the number of mammary lobes present. This has implications for mammary disease and the use of intramammary therapy. Fig. 10.1 Anatomy of the mammary gland. Cross-section showing major anatomical structures (lactating mare). Mammary gland development and the production of milk is a highly complex process requiring fine control and coordination of birth and mammary development; milk production needs of course to be coordinated closely with delivery of the foal. The process of the manufacture of milk is demanding of energy and requires a fully functional mammary cell structure free of inflammation. The process is largely governed by the interrelationships between the hypothalamus, the anterior pituitary gland, the ovaries, and the placenta. Several hormones are responsible for individual aspects of the development of the mammary gland and the change from a quiescent nonsecretory structure to a highly specialized secretory function which, in the first instance, produces colostrum and then quickly shifts to produce milk. • Estrogen causes development of the duct system. • Progesterone stimulates the development of the milk-producing cells but inhibits milk production. • Prolactin concentration increases dramatically in the last week of gestation and remains elevated until some 3 months after parturition.3 This increase is probably instigated by the cessation of release of an inhibitory factor in the hypothalamus.4 • The decline in progesterone at the end of gestation and the rise in prolactin over the last few days are probably the basis of the trigger for milk production to begin. • Oxytocin is secreted from the neurohypophysis of the pituitary glands in response to stimulation of the udder (usually by nursing).5 Oxytocin causes contraction of the myoepithelial cells and ejection of milk into the duct system and eventually into the teat sinus. Circulating oxytocin released during labor will also have an effect on the mammary glands, so milk may be ejected from the teats during later stages of labor. This may have implications for the quantity and quality of colostrum available to the foal. The so-called ‘milk let-down’ response can also occur in the absence of any detectable oxytocin in the circulation.6 Milk contains more calcium and potassium and less sodium than blood, and as parturition approaches these changes become more apparent in the mammary secretion.7 The concentrations of the various electrolytes in mammary secretions are used to provide information on readiness for birth8 (see p. 270). Milk is an ideal food material for the newborn and very young foal but becomes an inadequate total feed within a few weeks of birth (see Table 10.1). Low levels of iron and some other trace elements mean that a totally milk-based diet will result in significant metabolic deficiencies, and the energy requirement for the growing foal cannot be met solely by the volume of milk produced by the mare. Lactation is maximal at around 2 months postpartum, the average production in a Thoroughbred mare being around 10–12 kg/day. This production is roughly equivalent to 2–3% of bodyweight and should enable the foal to grow at a rate of around 1 kg/day. In order to produce this amount of milk the mare needs to be fed additional food value of 1.5 times the normal requirements for energy and protein. Mares that are deprived of food or which do not eat for other reasons will inevitably produce less milk in response to the deprivation and negative energy balances. In some cases (ponies in particular) the negative energy balance results in the mobilization of fat and hyperlipemia can develop. This condition carries a poor prognosis and is a relatively common occurrence in late pregnancy or early lactating overweight pony mares. Any overweight mare that is subjected to a reason for negative energy balance may precipitate hyperlipemia. The disease is not the sole preserve of overweight pony mares. This is not really a disease of the mammary gland but is supposedly due to rapid falls in serum ionized calcium associated with the onset of lactation. It is a relatively rare disorder of lactating mares and occurs within 10 days of foaling or 1–2 weeks after weaning.10 Stress (such as transportation) and mammary development together are particularly dangerous. • A variable increase in muscular tone, stiff stilted gait with hindlimb ataxia. Trismus (lockjaw) can be seen. • Muscle fasciculation (especially of the temporal, masseter, and triceps muscles). • Synchronous diaphragmatic flutter (abrupt spasm of the diaphragm at each heart beat, noticeable as hiccoughs or thumps in the costal margin). The signs are similar to those of: • Cranial (or major body) trauma. • Herpesvirus myeloencephalopathy. • Equine protozoal myeloencephalopathy. • Colic (particularly catastrophic abdominal accidents). • Treatment should be repeated as indicated from clinical and laboratory information. • Supplementary feeding of the foal for a day or two may be helpful in reducing the calcium drain. • Oral calcined magnesite may be used to supplement the dietary calcium. Alfalfa hay has a high calcium content and thus can be an effective high-calcium feed material. Stimulation of the parathyroid can sometimes be encouraged around parturition by feeding a low-calcium diet prior to the last 3–5 days before delivery and then increasing the availability of dietary calcium. • Poor body condition; physiological or psychological stress.11 • Fescue toxicosis.12 This pasture grass is associated with a high incidence of agalactia, thickened placenta, prolonged gestation, stillbirths, and occasionally abortion. Infertility at subsequent breeding is also reported.13,14 • Secondary to systemic illness including strangles. • Specific udder diseases such as mastitis and mammary neoplasia.
THE MAMMARY GLAND
ANATOMY
MAMMARY GLAND DEVELOPMENT AND MILK PRODUCTION
DISORDERS OF THE MAMMARY GLANDS
Eclampsia/hypocalcemia
Profile
Clinical signs
Diagnosis
Treatment
Agalactia
Profile
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree