Chapter 24 Systemic Immune-Mediated Diseases
Immune-mediated diseases may affect multiple body systems; for example, polyarthritis may be associated with thrombocytopenia or proteinuria. A CBC, platelet count, chemical profile and urinalysis are considered the minimum database for any suspected immune-mediated disease. The diagnosis of “idiopathic immune-mediated disease” remains a diagnosis of exclusion. Infectious/parasitic, neoplastic, and toxic causes must always be excluded with appropriate testing and/or therapeutic trials.
TREATMENT OF IMMUNE-MEDIATED DISEASES
Corticosteroids
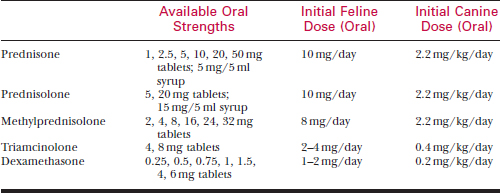
Therapy with an equipotent dose of a different steroid (prednisolone, methylprednisolone, triamcinolone, or dexamethasone) often resolves unacceptable side effects of prednisone (Table 24-1).
Combination Immunosuppression Therapy
Azathioprine
Chlorambucil
Monitoring of Immunosuppressive Therapy
Side effects of immunosuppressive medications often lead to significant morbidity; treatment of any immune-mediated disease involves balancing the control of disease against the side effects of immunosuppressive therapeutics. Obesity related to prednisone is very common, and owners should be specifically counseled about its prevention. Body weight should be recorded and weight management discussed at each recheck. Long-term immunosuppressive therapy may also allow the development of asymptomatic infection, especially in the urinary system. Urine culture is recommended every 3 to 4 months regardless of the absence of clinical signs.
IMMUNE-MEDIATED HEMOLYTIC ANEMIA
The diagnosis of immune-mediated hemolytic anemia (IMHA) is suspected upon discovering severe anemia in the presence of normal serum protein levels (Figure 24-1). IMHA may be classified as regenerative or non-regenerative with red cell destruction in the bone marrow prior to the release of reticulocytes. Red cell destruction may be mild (low grade) or rapidly progressive.
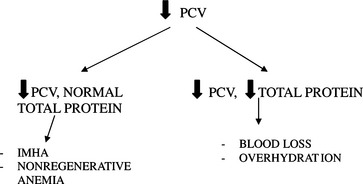
Figure 24-1 Classification of anemia. PCV, packed cell volume; IMHA, immune-mediated hemolytic anemia.
Etiology
Table 24-2 CAUSES OF HEMOLYTIC ANEMIA IN THE DOG
Hereditary causes (pyruvate kinase deficiency, phosphofructokinase deficiency)
Babesia canis, B. gibsoni, Mycoplasma hemocanis (formerly Hemobartonella canis)
Neoplasia (hematopoietic, hemangiosarcoma, histiocytic)
Microangiopathic (disseminated intravascular coagulation, heartworm caval syndrome)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


